Transcript
Hello, everybody. Welcome back to a master class series on the challenges of IFC staining. I’m Bettina Winkler from Visiopharm.
Today’s session will close a master class series, but we will continue to have webinars about how labs can improve sustaining quality and consistency.
So keep an eye out for this.
Closing the series is professor Ralf Huss. Ralf is board certified in anatomical experimental and molecular pathology with over thirty years of experience in international academic institutions and the pharmaceutical industry. He’s the CEO of the BioM in Munich, Germany.
Prior to this role, he was a founding director of the Institute for Digital Medicine at the University Hospital Augsburg.
Ralf will answer your questions after the talk, so please add any questions to the chat.
Ralf, over to you.
Good afternoon, and welcome to the master class webinar series. Today’s topic is the future of IHC opportunities and challenges.
My name is Ralf Huss, and here are my disclosures and affiliation.
I’m the chairman of the Visiopharm Scientific Advisory Board.
I’m pathologist at the Institute of Pathology and Medical Diagnostics at the University Hospital in Augsburg, Germany, and I’m also the managing director of BioM, the biotechnology development organization in Munich.
Before we dive deep into the applications of IHC and where the future lies, let’s revisit a little bit the history of IHC.
We are talking about more than a hundred thirty years of experience initially starting with the discovery of antibodies and increasingly more applications almost by decades. So more than a hundred years, we started on the use of antibodies in cytochemistry. And a hundred years ago, we started to understand the antibody antigen complexes, which are required to apply antibodies and understand the function of immunohistochemistry.
And then as you can see from this list, there has been an increasing improvement of technology to visualize the antibody antigen complexes over time. Later in my talk, and also during the previous master class presentations by our colleagues, we heard already about key I sixty seven and also on HER2 IC. But this already has a history of more than forty years where we learn more and more about the pitfalls and the opportunities, some of which we will discuss also during this presentation.
One of the first master class presentations came from Clive Taylor, a very experienced pathologist, and here is his abstract that you can also read from the master class series.
Immuno histochemistry entered the rear arm of diagnostic surgical pathology as more specific type special stain. Today, IHC is applied in anatomic pathology laboratories worldwide. With the advent of actual molecular biomarkers, IHC was pressed into services for detection and then quantification of such markers where the IHC result alone could determine therapy.
And for me, here comes the most important sentence.
In the latter, which means the determination of therapies, IHC is now repurposed from a stain into an assay. We have to move into a level of quality that is comparable to what we are used to in clinical chemistry for many years in terms of standardization and quality control. I’m in the practice of pathology for more than thirty years, and as long as I’m in this business, we are talking about this. But I think the time is now to implement that.
And Clive Taylor also phrased the term in cytoproteomics, which refers to the standardized quantification of antigens.
Explicitly on this topic, there have been recently a couple of publications that will change the practice of IHC. Here are just a few examples by Steve Bogen, and two by Clive Taylor again, referring to the quantification of the in situ proteomics, and improving also the standardization of IC.
I’m sure that we will see more of that. And one topic of this master class is, of course, can AI help and to what degree to assure quality assurance and manage quality control.
Here’s the list of the previous presentations from the Visiopharm master class webinar series.
The first one I already referred to, which was the one by Clive Taylor, IHC from a stain to an essay. But I will also revisit a couple of other topics that was introduced by other expert speakers, the technology of Qualitopix provided by Visiopharm, and what it means to integrate AI based quantitative quality assurance, what kind of tools like cell lines can be used for standardization and to standardize assays like Ki sixty seven and others.
And of course to understand inter laboratory HER2 variability, but also even intra laboratory variability, which requires the monitoring of immunohistochemical stains quality within a single lab.
And this will be mostly part of my presentation today to summarize some of those topics and revisit presentations of previous presenters.
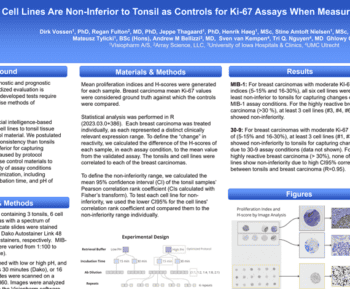
Ring Fulton talked about how cell lines are non inferior to tonsils as control for key s sixty seven assays when measured by image analysis.
So he proposed that this is a solution to standardize quality assurance by using robust cell line approaches.
Of course, there are also other solutions, but I think in most of our laboratories, we are still using in house controls.
And for us, the question is still open, which is the best control material, which refers to the performance of the single IHC assay on different stainers and different times of the day, and also other technical inconsistencies.
Paul van Diest talked about monitoring immunohistochemical stain quality with artificial intelligence. And here I’m also quoting his abstract from his presentation, presenting the results of an extensive IHC stain and stainer evaluation performed using Qualitopix.
The quantification of stain consistency enabled the lab to significantly improve their stain quality for HER2 and unveil staining variation based on their stainer. Something we also observed in Augsburg in a longitudinal study.
Another presentation came from Omar Baba. He validated an AI based analytical tool for IHC staining QA. And here is a post on the right side together with colleagues from Visiopharm, where it was used for precision studies of the digital pathology pipeline.
I think it’s worthwhile to revisit some of the presentations on the Visiopharm web page to get a deeper insight into these particular topics.
Let me now present a few experiences from Augsburg.
So we have started to implement cell lines as a control material for detecting workflow, and I call this workflow challenges, mostly in the pre analytical and analytical workflow area. I will come back to this in a little bit later, showing you how we integrate this into the entire pathology workflow with particular emphasis on IEC.
Here’s an example on key I sixty seven. You see screenshots from the Qualitopix software.
On the left side, you see the longitudinal measures of daily cases, where we’re using those cell lines to monitor the quality of key I sixty seven in our lab.
And you see the second dip in all four rows, where there is this circle at the bottom, which represents the view on the right side, where we looked at these cell line cores to understand why there was a lower performance and a less intensive staining for Ki-sixty seven. So this gave us a hint that we have to revisit and look into different variabilities of our workflow to understand why there was all of a sudden these drop in quality. And we were able to manage, as you can see on the left side, where Keyi sixty seven staining came back to normal quality in the following days and weeks.
Another example, and this is the first one on HER2, came also out of our Augsburg laboratory. I’m referring to the top line on the left side, where you see a drop in the three plus core.
And on the right side, you see once again the cell line control that we revisited after we had observed this drop. And you see already that there was an alert coming from Qualitopic software that alerted us that the stating of the three plus core was inadequate.
So now we were able to revisit this case, restained it, and made sure that all the ver variabilities were now at a proper quality, and we are back to normal staining.
So sometimes, as you know, as practicing pathologists and experts in the IC lab, some changes are very subtle, and you don’t pick them up immediately, and there is still a kind of danger that you don’t pick up the technical issues, and you might misreport a single case, which of course, may have an impact on the treatment for a single patient.
Another example from her too is on this page, where you see in this red frame on the left side, a drop in the two plus core, where we also received an alert as you see on the right side that there was an inadequate or a less instant staining for the two plus core and the for two plus staining, something we were also able to fix as you see on the left side again and all the further two plus stains as well as three plus and one plus were within the thresholds. But for us it is very important to see these longitudinal drifts and shifts in the staining quality, so that we can actually early interfere and understand where there might be an issue that we can then review in our laboratory workflow and check all different pre analytical and analytical steps.
The last example from Augsburg is a case on PD L1.
And here you see even a more dramatic shift towards a false negative staining, at least something that we interpreted as such, where you see all of a sudden a drop in the staining intensity of PD L1, which was also supported by the analysis of the cell line course on the right side.
So we checked the antibody and eventually had to change the antibody source to come back to normal staining intensity, which is, as you know, in p one, it’s not so much about the intensity, but it’s definitely about picking up the right percentage of PDL one positive sales, especially around different threshold levels. So in summary, after having revisited now Ki sixty seven, HER two, and here PDL one, the AI supported system Qualitopix by Visiopharm in a long longitudinal observation and use in the lab was for us very helpful to early pick up shifts and changes in staining quality, but also be able to detect single case changes that still has an impact on a single patient treatment.
Let me go back to the process and the process optimization of a standard histopathology workflow.
The central line is the classical steps in a workflow from sample all the way from sample management into the reporting, which has different steps of course like grossing, cutting, and eventually scanning and reporting.
So we developed and this is a very rough plan, we have this in way more detail, how we can integrate image analysis and digitization including AI into the different steps.
It is of course very difficult to control all the different steps, especially those at the incoming end of samples. It’s difficult to standardize of course the fixation time, the range of the tissue specimens to the volume of the fixative and others.
And also grossing depends on the experience of the pathologist.
But, of course, we are making tremendous efforts to also standardize all those steps. But what we are definitely be able to control, and at least to assess from a image analysis point of view with AI support, is the issue around staining quality and scanning. So that before we send this report out and these images out, there is a check-in terms of quality, which, of course, raises a lot of confidence to the pathologist that the reported result is of high quality and not due to any kind of workflow, inconsistencies, and maybe even an error.
Let me briefly touch on two topics.
The first topic will be on the h and e staining and the second one on some scanning issues, which all, if I’m now jumping a little bit ahead, can of course be resolved.
This is a very interesting and recent paper by a group from Leeds in England, where they showed that depending on the different stainers or even from the same vendor and a change in the incubation time of agent, e agent definitely changes the staining intensity on the same type of tissue, which is here a liver specimen.
Of course, the different staining intensities is not so much an issue for us pathologists, we can cope with that during the manual read. But of course, this becomes more issue if we will use AI based diagnosis and AI based decision support even on H and E, on which some companies are actually working, which definitely is more a type of issue is the what I call scaling issue. There are many scanners on the market. All of them have a high quality, high throughput, but depending on the lenses and the type of the adjustments, you will see from the same type of bone marrow specimens that we used here, you do see different resolutions and staining intensity.
Once again, it is not so much an issue for menu reads on a screen, but the moment you apply AI and image analysis based decision support, any kind of blur area or other issues and staining inconsistencies definitely has an impact on the results reported and supported by the AI. But these are things that will be standardized and I’m very confident that this will be also resolved in the future.
But since we still experience some of the issues we published this workflow diagram about four years ago in the journal of pathology. This is in principle a workflow diagram that starts with stained tissue slides either monochromic or multiplex staining even IF. At every step of the process there is a slide QC which can be done either manually or automated by image analysis and with AI support.
At the time of transition going from a manual read into a fully automated reading with increasing more standardization, it is still necessary that we are able to control each and every step of the development which is depicted here.
So at every step the Pathologist or the Lab Manager can decide that this staining is adequate and can use AI measures to assess and evaluate the staining quality and pick up trends, as I was trying to show you during our Augsburg experience.
Of course, time has passed. We have published this diagram in twenty twenty three together with Bharat Yasani and Clive Taylor.
What we would like to see in the future, which we call here the beauty, is that we can use artificial intelligence, including data integration with other metadata and patient data to make educated decisions on treatment decisions based on robust biomarker detection also in multiplex assays.
But this, however, requires that we can manage the beast, which were all inconsistent results based on generated artifacts at any ways of the workflow, that incorrect results lead to false classifications, or that we even find pitfalls like irrelevant results in a meaningless context. To manage the beast, I’m very confident that we will be able to use AI supported quality management in the future that gives us more confidence in the results and also increase the credibility of AI based tools and IT and digitization in the pathology.
At the end, let me thank my colleagues from Augsburg, Claudia Herbst, Johannes Raffler, Joachim Bakos, and Bruno Merkel, and of course, the entire Visiopharm for close collaborations and support.
Thank you very much.
Thank you very much, Raif.
I’m sorry. I I see my screen. I see myself, on the screen, but I don’t know why you don’t see me.
So the first question is coming in. What are the alternatives to Qualitopix? Is it a case of Qualitopix versus living with stain inconsistency?
No. I don’t think that we should live with staining inconsistencies. I mean, this was something I was trying to to explain and to rationalize. This is in the future and also based on the increasing regulatory framework that we experience.
I think we need to document any kind of staining inconsistencies. As I was trying to say, it’s, of course, very difficult to control all the pre analytical issues. I mean, we are already doing this. I think most of the pathology department is doing this as as well, that we are providing the fixation material.
We try to control the fixation time. We try to document everything.
And, so I think we have to even increase or or broaden the applications of a quality control and quality assurance measures all the way from the incoming results until we report that.
And, so I think, there is no option in the future to live with staining inconsistencies.
And a little bit as a side remark, something that that I very much like, I we we play a little bit around with with explainable AI to really understand how those those algorithms come up with the solutions. And for me, it was sometimes an eye opener how we as a pathologist doing the job for thirty years, sometimes come up with decisions.
This is, sometimes we look at areas where there is where the the algorithms, the image analysis don’t even look at. And I think we have to con converge this knowledge and this information. So for me, there is no option to basically cope with with staining inconsistencies in the future.
Okay.
That’s fine.
See my my screen? No. Sorry for that.
K. No problem. We have another question coming in. How difficult was it to find the root causes of the inconsistent test results?
Now this is a very important question.
Sometimes it was it it was actually sometimes difficult. Sometimes it was very easy. But in in the single case with Ki sixty that I was showing you, it was just a mechanical issue that we had on on some of the the stainers.
For the HER2, we eventually had to replace the antibody, change it to a different antibody that we were using.
So my hope is, and, I think this is what what most colleagues are also waiting for is that you also get, let’s say, a troubleshoot list like you have in your car. The moment, you know, it doesn’t turn on, then you get this this check, that your the car mechanic does on your car and gives you gives you a a list of of possible results. And this is something that we also hope for. And so we we collect more and more experience that when we see a sudden a sudden change in the long material documentation of the staining, which is which is quite different from if there is a a tendency an increasing tendency.
And something that I would like to stress is also that for me, who is doing this for for many, many years, I mean, in trying to be self critical on this issue, is that a hurdle that we we look at on Monday mornings, we might be interpret different on a Friday afternoon, which, of course, we would officially never admit. And we it should not be the case. But I think there is the human factor is still here in in the game. And this is why we do, of course, a, we we always report those cases with with another colleague who has a maybe not this personal bias.
But this is something that we definitely hope for that these kind of of longitudinal documentation allows us even to pick up subtle changes that we cannot see by by plain eyeballing and which we sometimes can interfere early on. So it really is a is a matter of collecting experience, but something also that we will in the future use AI for to give us a, let’s say, a troubleshooting, menu guide. It’s not a menu guide. It said there would be a digital guide, but it some some kind of troubleshooting guide.
That would be good.
Yes.
Next question. Without published data on the downstream consequences of staying inconsistency that I know of, how can labs evaluate the value of Qualitopix?
Honestly, there is there’s actually a lot of data on on the the reasons for preanalytical inconsistencies, and this is why we are trying to standardize that. So I think the more we use standardized controls like, you know, cell line controls, like like other controls instead of, let’s say, our own tissue, like we do sometimes on an appendix, the placenta, tonsil, whatsoever, depending on the, on the the case, that we are doing is I think Qualitopix is is already a very important core technology in this because it gives us it gives us information already on the on the staining and on the the staining devices. We have three ICs staining from the same company.
And what we realized is that in some instances, one stainer had a different performance than performance than the other. And even putting it in a different rack number has sometimes a different performance, which is usually not an issue. But in some cases, it might be an issue. You you can pick it up very early on and longitudinally.
So I think we have to extend this quality control, all the way into the the early sample entry and and sample management all the way to the reporting. And I think every lab in the world does the utmost to to control these these inconsistencies.
Okay. Perfect.
There’s another question from Bert. You mentioned DataFlex as a collaborative effort. Beyond this, what was the initial experience with QC management and ease of adoption?
It takes an effort. It it takes time and effort to convince, particularly your lab personnel, to adopt this because it changes the workflow. What we did actually in this diagram that I was showing you, this workflow, we asked our department of the of our university, which usually just does to workflow analysis in, the automotive industry and in other areas to go into a pathology lab. They have never entered a pathology lab before.
And all of a sudden, they came up with with information that we, for example, passed the same door three times in one minute for no reason. That’s just the reason. Just because we did it this way for twenty years. So it takes effort.
It even takes sometimes money, but we we strongly believe in the fact that this is worth the effort, digitizing your lab. Every time we experience that the moment it works, the moment we saw the changes, everybody was accepting this kind of effort and is is is willing to to go the extra mile initially, it would make makes it easier in the end. So like everything else, initially, you need a catalytic energy that you have to put into a new process.
Mhmm. Great to phrase it.
Next question is from Matt. How do you see the role of EQAs evolving in the future?
I think giving the I wouldn’t call this pressure, but I think giving the the increasing role to to document the staining quality and the quality of all the process in the lab, I think EQH will play an increasing role to give us guidance in the lab how to implement different steps. There is not the the only way, but I think we need to, to to get guidance. We need to understand that we need to improve our intra and inter laboratory consistencies. We need to document this.
This is a matter on, providing the best diagnosis and the best options for treatment decisions for the patient. Because as we all know, the diagnostic world, particularly the world of the diagnostics and and making therapy decisions as based on on tissue based biomarkers is increasingly complex.
Not only PDL one, but but also others. And it took us twenty years almost to adopt HER2. And I think we don’t have the time and the expertise. And given the the limited number of pathologists worldwide, I think we need assistance to cope with this increasing complexity, and EQA EQAs will give us guidance and and help us with this.
Okay. Perfect. So thank you, Ralf, for this really insightful talk and the q and a session. Bye, everybody.
Thank you. Bye bye.
In his lecture, Dr Huss will summarize the previous highlights of this extraordinary Masterclass from the need for quality control in precision pathology to the implementation of an automated and AI-based solution in a routine pathology workflow. With a special emphasis on the value of AI in controlling the robust performance of standardized IHC assays, Dr. Huss will advocate the importance to IHC tests to be acknowledged as an assay without increasing the burden on routine histopathology laboratories. On the contrary, such an approach could even compensate or at least forecast assay failure which allows early countermeasures from pre-analytical to post-analytical errors.

Prof Ralf Huss, BioM Biotech Cluster Dev. GmbH & University Hospital Augsburg, Germany
Ralf Huss is a Professor of Pathology and currently the Managing Director and CEO of the Biotechnology Development Agency in Munich, Germany. Prior to this role, he was the founding director of the Institute for Digital Medicine at the University Hospital Augsburg, Germany. Dr. Huss is board-certified in anatomical, experimental, and molecular pathology, with over 30 years of experience in international academic institutions and the pharmaceutical industry with a focus on histopathology, immunology, cancer research, and digital medicine.