Transcript
Welcome to the master class series on the challenges of IHC standardization.
Today, we are proud to present the first master class by professor Clive Taylor.
Clive is widely recognized as one of the founders of the fields of immunohistochemistry.
Over his career, he has been a leader in research, clinical, and in industry, as can be seen from his presentation today.
The presentation will take about forty five minutes and will be followed by a q and a session.
You can share your questions in the chat during the talk, and they will be taken at the end. With that, I want to hand over to Clive for his presentation.
Thank you, Dirk, for that introduction.
My name is Clive Taylor, and welcome wherever you are in time or place to this first in the master class series.
My title will be Precision Medicine Demands Precision Pathology, and the theme will really be IHC immunohistochemistry converting it from a stain to an assay with quantification features.
And my argument will be that the time to do this is now. So my charge here is to set the scene for more detailed discussions that will follow in this master class series.
Now any test in the lab, every test in the lab, is shaped by four main factors from the past, the present, and the future, in fact. There’s the background environment in which the test is being used.
There’s the current operating environment, what is done today with the test.
The needs or purpose, what do we actually want to do, and then the march of technology, what can we do, what might we do tomorrow.
So part of this, presentation stems from an opinion article that Barbara Jean Manjani and and myself wrote a few months ago, appeared in archives pathology, that immunohistochemistry should be regulated as an assay, not as a stain.
The background really is that fifty years ago, IHC entered surgical pathology, and was used as a more specific type of special stain, a PAS or a trichrome or something.
And today, IHC is applied in that role in anatomic pathology worldwide.
With the advent of actionable molecular biomarkers, IHC was pressed into service for a different purpose, for detection and, in fact, quantification of these markers, whereby the IHC result alone could determine therapy. Does the patient get treated or not?
In this latter application, IHC was effectively repurposed from a stain to an assay, but unfortunately, the necessary pre analytic, analytic, and post analytic changes that would accompany this repurposing did not evolve a pace, and this resulted in poor clinical performance.
Today, key technologies have evolved to the point that some of these deficits may now be addressed, which would transmute IHC from a stain to an assay, something that I’ve like to call in situ proteomics.
So let’s look at the background in which IHC developed, some key milestones.
A long time ago, around eighteen fifty, I would argue that the microscope the availability of, improved quality lens preparation, reduced the cost and availability of such that some clinicians, some surgeons began to spend more and more time with a microscope, less and less time in the operating theater, they in fact became the first anatomic pathologists.
About fifty years later, the studies of diphtheria or antitoxin led to the general understanding of what antisera were, and then fluorescent labels were applied to antibodies or antisera on frozen sections, and the fluorescent label was eventually replaced by an enzymatic label, immunoproxidase, to transfer this method to paraffin sections. And about the same time, Milstein and Koller in Cambridge invented the technology that led to monoclonal antibodies.
And then the year two thousand saw the advent of molecular biomarkers and the beginnings of true digital pathology.
Number of the slides that I’ve shown and, and background information can be found in a couple of books that I was part of editing. The first was called From Magic to Molecules, a History of Disease and Pathology edited by Jan van den Twil, a good friend who’s now deceased, unfortunately, Jan Gu in Beijing and myself, and then more recently, Precision Cancer Medicine, the role of a pathologist and, in fact, to a large extent, the role of AHC by Bharat Chasani, Ralph Hulse, and myself up from Springer in in twenty twenty one. So, eighteen fifties, surgical pathology was just beginning, as I’ve mentioned, and two individuals, James Padgett and Rudolf Virchow, got their primitive microscopes and looked down them and said, well, with my microscope, I can see cancer.
And the era of surgical pathology began, and they both, in fact, illustrated cancer cells that they saw, a hundred and seventy years ago, and the illustrations are still good enough to show to students today.
And somewhat sort of by serendipity in the background, this process was assisted by the dye and clothing industry and by a tree in Honduras called the hematoxylin tree.
And the dye and clothing industry plus hematoxylin led to this standard stain that we know today as the hematoxylin and eosin stain, and that in fact became the gold standard for diagnosis of many diseases by about nineteen hundred.
However, many conditions then and now were concerned that morphologic diagnosis of cancer and other diseases was, in fact, very subjective.
For example, here are six anaplastic tumors and whereby the exact diagnosis, if if you show them to different pathologists, becomes a matter of opinion. And six pathologists might give similar or different answers.
One French clinician, Marcel Basis, gave his opinion of what he thought of the science. He said it’s about the same scientific level as collecting butterflies. Sure. It’s a science, but maybe it’s not one that we should base diagnosis upon.
Nonetheless, in spite of the misgivings, H and E was the gold standard for a hundred and fifty years.
On a form of paraffin section, the diagnostic opinion of a pathologist was final.
There were, however, attempts to improve objectivity. And as I’ve mentioned, about eighty years ago, antibodies were labeled with fluorescein and applied to frozen sections. Albert Coombs used them to look for streptococcal antigen, and Astrid Fragrass in Scandinavia used, immunofluorescence to look for immunoglobulin in plasma cells.
These methods were excellent in terms of detecting antigen, but they had limited use in anatomic pathology because the fluorescence method requiring dark field microscopy, in fact lost the gold standard of morphology, and so pathologists in anatomic path did not accept the method widely.
A few years later, we simply were working with Ian Burns and David Mason in their lab in Oxford, substituted the fluorescent label with an enzymatic label, peroxidase, and this led to the immunoperoxidase method, which in fact combined immunology with morphology. We could apply the method to look for plasma cells, as we see on the left, in a form of paraffin h and d section environment and retain the morphology.
So we published a number of papers about it, but recognition of IHC or use of IHC, struggled because most of the papers from other labs, in fact, tried to prove it didn’t work.
And it stayed that way to some extent until a seminal paper in nineteen eighty five by one of my students, Kevin Gatter, at the top and a good colleague and friend, David Mason, with whom that the most of the initial immunoeproximate studies were published.
They looked at a hundred and twenty consecutive routinely processed biopsy specimens from the Oxford pathology department of anaplastic tumors or tumors of uncertain origin.
And using simply cytokeratin and common leukocyte antigen, they showed that the morphologic diagnosis was actually wrong in fifty percent. That’s an astonishing number, and it had a huge impact as you might imagine.
Same day that this paper appeared in The Lancet, I had a little postcard come in the mail. I was in California by then, and, it said, the clever men at Oxford knowed all there was to be knowed, but none of them knew half as much as intelligent Mr. Toad. That, of course, was from Wind in the Willows, Kenneth Graham, who sat on the banks of the river in Oxford and wrote that. And David Mason, of course, was a was a humorist, and he sent it, and he actually published that too, so to as a comment on anatomic pathology.
So what that paper did was it was the first dramatic demonstration that IHC was important, indeed essential for diagnosis of anatomic pathology, at least in relationship to anaplastic tumors.
And it led to growing acceptance and use of IHC for hundreds of different special stains, almost as many stains as there were antibodies on form and fix paraffin embedded tissues.
Now what’s important to realize is that we used the same rationale back then as for any other stain.
That is the goal was simply to produce a different color to assist cell and tissue recognition for the purposes of diagnosis.
Nothing more, nothing less.
But over the past hundred years or so, that approach led to some very bad habits that we still are struggling to cast off.
So on the left, we see three HNEs from the same block, sections from the same block, sent to different leading labs around the country. In a study that the FDA did with the Biologic Staying Commission in the nineteen nineties, concerned about the the, general quality of staining and the reproducibility of staining.
And it was really recognized by FDA and and the Biologic Staying Commission that the HNE has has essentially no controls other than qualitative controls. The result is adjusted to please the pathologist, and you can see those three HNEs are actually fairly different, very different from one another. But they were those chosen by the pathologists at those three different institutions for diagnostic purposes.
And if one wanted to get this to be more reproducible, then controls would be necessary.
So it meant that for H and E, reproducibility, in fact, is poor run to run, day to day, and certainly from lab to lab.
And on the right, there’s a a special stain, IHC for CD thirty.
It should, must, in fact, have positive and negative controls, and it should not be adjusted to please the pathologist. But unfortunately, I’ve observed numerous occasions of it being adjusted exactly to please the pathologist who will say, hey. It’s not quite dark enough. I’d like this to be a little darker, and the tech will tweak it, longer incubation, higher concentration of antibody, whatever, to produce the result that makes their boss happy.
Result, of course, is that IHC has overall poor quality quality.
It’s variable. And of course under those circumstances, quantification is impossible.
So reproducibility was poor, and it really became an issue as as to why is that.
Early on, it had been thought that it maybe was variability in the antibody or fixation, but it’s it is those two things, but it’s also everything else.
And in nineteen ninety two, the FDA and the Biologic Staying Commission had a a weak, symposium that they investigated and studied the reasons for this.
And in fact, it was everything, and this led to the total test concept for immunohistochemistry borrowed from from the clinical laboratory. What mattered really was the clinical test question, what you’re trying to do. Specimen acquisition was critically important. The analytic issues, the protocol, the qualifications of the staff, interpretation, the validation, the reporting, the controls, and the final interpretation and reporting, all of those things were critical.
They needed to be standardized in order to get a standardized result.
So having recognized that, where did that leave us? Well, by the year two thousand, the gold standard was still the h and e. And we had on top of that forty years of immuno chemistry, which basically was forty years of bad habits.
But then twenty five years ago, two things happened that changed everything, and in fact forced a number of changes that we’re still struggling with. The first of these was that the first companion diagnostic was approved by the FDA. This of course was the Doc Murray at Daco said, here. Go ahead. This test is approved as a companion diagnostic for use with Herceptin, the drug.
So IHC suddenly was pressed into use to do that.
About the same time, fortuitously, radiology went digital. This was a technologic advance.
And as a side effect, to handle these large radiologic images, the PACS system was introduced into most hospitals. Picture acquisition communication system, it could handle large digital files, and it made it possible to begin to transfer, transmit digital pathology files. So digital pathology within was enabled by what happened in radiology.
Now through this process, immunohistochemistry was dragged into the era of precision medicine.
If we look at the four pie charts at the top here, the top left is the traditional morphologic subdivision of lung cancer, adenocarcinoma, squamous, non small cell, etcetera.
Clinicians were telling pathologists that morphology alone is not enough, send a diagnosis in two thousand and eight to our pulmonary surgeons that this was simply small cell carcinoma of the lung, and you get an answer back, I’m not really interested in what sort of cancer it is. I want to know what the actionable biomarkers are. And by two thousand fourteen, there were lots of them. At the top right, we see a pie chart for adenocarcinoma of the lung, and there are a dozen or so actionable markers.
That’s in two thousand fourteen. Today, there are, of course, many more. And it also extended to colon cancer, melanoma, and, in fact, most types of cancer. And these pie charts are from a study by Zhang Gu, and myself almost ten years ago, and, of course, there are more markers.
And now it’s really clearly established that morphology alone, at least in the instance of cancer treatment, is not enough.
Precision medicine requires precision diagnostics.
Now it turns out that met many of the targets, for personalized therapy are in fact proteins, and IHC, of course, in theory, is an ideal method for detecting proteins and potentially for measuring them. But to do that, we need to improve IHC performance, particularly the choice of controls and particularly the interpretation of the results.
So so what’s the problem?
IHC detects the targeted protein, but it’s just a stain.
Can we achieve the consistency and the quality to turn IHC, the stain, into a quantitative assay, and in fact reach in situ proteomics, that is the measuring of protein per cell?
Is it possible to take a HER2 result, which simply today is scored as plus, two plus, three plus, or zero, and turn that into a result that’s quantitative as per example, the number of attagrams of HER2 per cancer cell on average.
What would we need to do that to convert a stain to an assay? Better validation, better controls, calibration controls for sure, and interpretation must be much more rigorous than it is today.
And the problem, of course, is in the details. There are many uncontrolled variables, and can we do anything about it? We’re beginning to recognize what they are.
The scoring of predictive markers today is crude. I’ve already mentioned HER2, zero, one plus, two plus. And if we see a score and somebody’s calls it one plus, is that score in fact real? Does it reflect the biology of the cancer? Or is it due to some variation in the test the total test process?
Sample preparation, variable section thickness, variable protocols, different antibodies, different labs, different chromogens, heterogeneity in the section, and variation in the pathologist scoring.
It could be any or all of those things, and the only way of distinguishing which it is and standardizing it is better controls.
The extent of the problem, in fact, is astonishing. Here’s here’s a a slide showing Nordic QC and UK Nikas results. These are two external QA programs in Europe, one in the UK, one emanating from Scandinavia. They they use worldwide.
Run ninety six had three hundred and sixty five participants, whereby each participating lab has sent two unstained slides from the same block, and asked to stain them internally, in this case, for smooth muscle actin and for cytokeratin.
Look at the huge variation.
Heat retrieval was used in two hundred ninety seven labs. Seventy six percent of those got acceptable results. Use enzymatic retrieval, and only twenty nine or thirty two percent got acceptable results. So there’s a clear message there. Don’t use enzymatic retrieval.
Then look at the primary antibodies.
In these three hundred and sixty five labs, twenty six different antibodies were used by sixteen different suppliers. There’s no cross correlation, cross comparison with these antibodies. It’s astonishing that the results are as good as they are, not surprising that they are as bad as they are. Detection reagents, twenty six reagents, thirteen different suppliers. Some of these were done manually, most by auto stainers, but by seventeen different instruments from seven suppliers and the Chromagen from nineteen suppliers.
Given this incredible variation in the background, as I’ve already mentioned, it’s astonishing and a compliment really to pathologists that it’s as good as it is.
Now when I was serving as chief editor of applied immunohistochemistry and molecular morphology, I invited Steve Bogan to give a clinical pathologist perspective on all of this, and he was already working on the on, on better control systems. And he did a root cause analysis of the error rate. The table on the right shows the findings for HER2 and and some ERPR results. And look at the astonishing discordance rate.
It varies from three percent up to almost seventy, seventy four percent, discordance for the same test in different labs. In the clinical lab, this would cause the lab to be closed down. In anatomic pathology, we need to be more attentive to what happens. The study was conducted in such a way that that the issues that were focused upon were analytic issues, not the pre analytic issues of, fixation, which remains part of the problem that I’ll address in a minute, and not the interpretive issues, which, again, I’ll address in a minute.
So we’re part of the problem. Right now, immunohistochemistry has elements of witchcraft in it. That is each lab does its own magic thing. Here’s the lab manual for our lab, with no apologies, and here’s the chief tech coming to work.
So, you know, it’s it’s magic. We do well, but we don’t do well enough. It leaves the big questions. Can we improve the quality to the point that we can get to quantification?
We would require detailed strict protocols with standardized controls that we all share.
And once we have those, it will require that we follow the protocols exactly. No more tweaking allowed.
And we require better controls for better QA, and we require calibration controls, because without calibration controls, quantification is not possible.
So the question of what is the ideal control is not a new one. It’s been asked before. There was a seminar symposium held at the National Institutes for Standards in in Washington, n I s t, way back in two thousand and four. It was attended by the FDA, by the Center for Medicare Services, who pay for these tests, so they were interested, by the Biologics Staying Commission and by a gaggle of experts.
The conclusion at the end of that, I focused on poor results for HER2 ER and PR, was that standard requirements for reference standards in IHC should include that the control must be subject to the same rigors of sample preparation as the test tissue.
It should be integrated in all steps of the test assay, including evaluation of result. It should contain a known amount of the reference standard protein, I. E. It should be a calibration control. It should be universally available, and it should be inexhaustible and inexpensive. And, of course, there is no existing control that meets all of those requirements today. But by combining one or two or combining two or more of these control types, we can get close to where we need to be.
What choices do we have for controls today, the existing controls? Well, upper left is the internal tissue block, both a selected positive and a negative, that is the standard control process in most AP labs that are doing immunohistochemistry.
Now in doing that, we need to recognize and clearly state what is usually just sort of swept under the table is that it means that every individual lab is in fact using a different control.
We don’t use the same control in our lab as you do in your labs, and none of the two of you or none of the many of you use diff use the same controls. You all select an internal block, all of which have been processed differently, all of which have different amounts of the protein in question. And we are therefore standardizing our internal test to different controls. So it’s not surprising that the tests are variable.
Sausage blocks, which some people like to use, or microtissue arrays are in fact in many ways worse because each of those cores, in fact, has a different pre analytic phase. They’ve all been fixed slightly differently.
Cell line preparations, in theory, could produce a standardized control that we could all share. It’s difficult to standardize the amount of the antigen of interest in in cell lines, and the morphology, of course, is different.
At the bottom, we see faux tissues or pseudo tissues or histoids.
The left of those two is a true case of breast cancer stained for HER2, and the right is a faux tissue of breast cancer cell line and fibroblasts that, resembles true breast tissue and even has the same morphologic features. So it’s great for morphologic comparison, but, again, it’s difficult to produce a standard known amount of HER2, in this case, in those cell line preparations.
The only cell control only control we have that can be standardized for amount is based on the peptide protein type controls, published a long time ago by Sampura Monell, that’s Steve Bogan’s lab, that, evolved today to the peptide controls that are gonna be discussed later in this master class series.
So this figure in the paper root cause analysis by Steve Bogan illustrates the the peptide controls, which basically is a synthesized peptide attached to the surface of glass beads at known concentration with a known amount of fluorescent label so that the intensity of stain of the glass beads, the intensity of fluorescence, can produce an exact quantification as a calibration for the amount of fluorescent seen for the corresponding antigen in a tissue section. So these have the potential to be calibration controls, and work is ongoing on standardizing and broadening application of this system, and that will be discussed later in the series. You need permission for this figure, so thanks Steve for permission.
So the end result here really is that we sort of, are moving IHC as an anatomic pathology test, and we’re borrowing or attempting to borrow from what happens for the ELISA test in the clinical lab. Now ELISA is enzyme linked immunosorbent assay. It was a test that evolved at about the same time as IHC did, you know, fifty years ago, and can be used to quantify the amount of antigen protein present in a fluid.
IHC and ELISA use the same reagents, essentially. They use an antibody against the target antigen, maybe use a labeling antibody, and they use a, an enzymatic signal, in this case, peroxidase.
ELISA releases the signal into the test sample fluid, and the intensity of color of that signal directly correlates with the amount of antigen present such that ELISA has excellent reproducibility and is strictly quantitative.
In ELISA, the sample preparation is strictly controlled. If the sample doesn’t meet those control requirements, it’s rejected.
The process is fully automated. It cannot be tweaked, and there are universal reference and calibration standards such that every lab works against the same standard and results are therefore comparable, strictly comparable from lab to lab. Compare that with immunohistochemistry where sample preparation is largely uncontrolled, the process is only partly automated using all sorts of different systems that aren’t cross correlated, and there is no universal reference standard. In fact, each lab works to a different standard. The result is poor reproducibility, and it’s not quantifiable.
So the answer is simple. Simply convert the requirements of ELISA to IHC, and we would, in theory, move to excellent reproducibility and quantification, and that in fact really is what is happening in the background here in a simple sense.
So what do we need? To assure quality and quantification and reproducibility?
Well, the current control systems that we’re talking about will control for the analytic process, the primary antibody, the secondary antibody, the label, the chromogen, the method, the protocol.
And in retrieval is sort of sometimes regarded as part of the assay, it’s also in a sense part of the pre analytic issue, and it is a variable, so it also must be controlled because different labs use different AR.
And we still have to address fixation, which is outside current control systems, and the readout or interpretation, which also is outside current control systems.
Now once we get to the point that calibration controls are, in theory and practice, able to assure action, it may then be possible to quantify a range of internal proteins as internal controls because molecular biologists use internal controls routinely.
The amount of actin, for example, actin RNA DNA as a control system for when they’re measuring molecules in tissue extract environments.
I presented some of this stuff at Caltech ten years ago, and the simple answer is why aren’t you using internal controls? Thinking about it, my answer was, well, yes. We sort of are, but not in a quantitative fashion. For example, way back in nineteen seventy four with Ian Burns, our first paper, we used plasma cells, kappa versus lambda, as internal controls one against another.
Hector Batafora went a step further in the nineteen eighties, advocating the use of vimentin as an internal a general internal control.
His rationale was that if you could stain vimentin, then it meant that at least some proteins had survived the pre analytic process.
And in a more precise way, when we do estrogen receptor, if we find a cancer that’s totally negative, as in the bottom left image, then we don’t know if that’s biologic negativity or an artifact of fixation or the analytic process. So we cast around to find a residual normal breast duct. And if that’s positive, it at least tells us that the assay that worked, that the fixation was fine, that the process is likely valid, and the cancer therefore is probably a true biologic negative. So that’s a precise use of internal control, but still not at the level of quantification.
So let’s assume that we’ve done all the things we’ve talked about, and the method is the best that we can make it. We’ve then sort of moved it from a stain to an assay. It’s not just a stain anymore.
And it leaves one remaining problem, a large problem, and that problem is us, the lack of objectivity of the pathologist in reading these things.
Now I’ve argued, presented the notion, if in fact, that a hundred and fifty years ago, better microscopes invented the original old pathologists, the morphologic pathologists. I think the same thing is happening today, that digital imagery, digital pathology, artificial intelligence is inventing the new digital pathologist. I think we’re not all realizing that, but it’s happening, and I believe that it’s inevitable.
So if we go back to the PD L1 test, this is one of the most difficult IHC tests, existing.
It’s a class three approved by the FDA test, meaning the result can stand alone.
And this paper here, published in AIM back in two thousand fifteen, Teresa Phillips et al, who’s one of the coauthors, demonstrates the extreme length that daco slash Agilent went to in producing a validated test that met the FDA requirements.
It was validated against the clinical outcome, the clinical study, which cases responded to PD L1, which ones did not.
The FDA required that the assay had a validated method, validated each reagent was validated. The controls were validated. It had cell line controls, and the scoring was validated.
It was manual scoring in this case, and it meant that the pathologists using the test had to be cross trained and repeatedly retrained.
Even then, it was very difficult to get a standardized readout.
The challenges are worth looking at. There was the challenge of identification in the scoring of the cancer cells.
Even when we scored them, it was a a percentage, not true quantification of the analyte.
In some tests, it was also necessary to identify and score and separate the immune cells, and all of this meant that reproducibility was, to say, the least challenging.
Here, for example, are four PD L ones.
Which is negative, which is positive, which one should be treated, and what about the immune cells, and which threshold are we using, one or five percent or fifty percent?
Let’s just look at the percentage issue. We might think it’s easy, but in fact, this is very challenging.
Percentage requires counting the number of cancer cells that show positive staining and essentially dividing that by the total number of cancer cells and doing that by I. So percent positive cancer cells over total cancer cells.
In a tissue section or a whole slide image that might measure three by two centimeters of sample prostate, we can have up to two million cancer cells in the tissue section. Two million.
Now Now we don’t look at the whole section, we look at a field, so let’s calculate the number of tumor cells by pi r squared if they’re averaging twenty microns in diameter in individual fields.
We tend to score times twenty or times forty fields by immunohistochemistry.
In a times ten field, there would be a potential of ten thousand tumor cells if they’re confluence throughout the field. And in a high power times forty field, there could be up to six hundred cancer cells if they’re confluent. And, of course, the number will vary according to the mix of tumor versus stroma.
We put down a number, but have we actually counted those cells? No. We haven’t. We’ve made a guess or a guesstimate.
So let’s look at that and the impact of that in just one hypothetical example. Here’s a times forty field. We’re looking at PDL one. We’ve got a threshold of five percent for whether the patient gets treated or not. So one high power field, we need the positive cancer cells and the total number of cancer cells.
The total number would be the denominator. We can’t actually count the six hundred in that field, so we make a guess. We say, well, we think the maximum would be six hundred.
Looks like about half of these are cancer cells, so three hundred cancer cells, and the denominator, therefore, would be three hundred. We now need the number of positive cells to get a percentage.
It’s a membrane stain, so we count the positive cells. Fifteen cells would mean we’ve met the five percent threshold, and the patient would get a hundred thousand dollars worth of treatment. Fourteen cells, no treatment.
Anybody think you can actually do that? I can’t.
And even worse, if we’ve got the denominator wrong, if it’s actually actually three hundred and thirty cancer cells, not three hundred, or two hundred and seventy, not three hundred, then the number changes to determine whether treatment is given or not. And even worse, if we do that on one high power field, we may have looked at much less than point zero one or even as low as point zero zero three percent of all the cells present in the section. So this is not a good test.
And there’s a second problem, distinguishing the cancer cells from the immune cells.
Positive cells, the numerator.
On the top, we have an adenocarcinoma.
That would give us the numerator, those positive cells. Most of them look to be positive, so we’d get a number to put above the line. Those are the positive cancer cells, except that if we now do a phenotypic identification using CD68 for macrophages, we can see that forty percent or more of the positive cells in fact are macrophages, not cancer cells.
So our numerator would have been inflated by a factor of two or more.
Wrong result.
Bottom case. Is this a positive test? It’s a squamous carcinoma. Does it meet the one percent or five percent threshold? I showed the actual glass slides of this case, to a group of pathologists that we were training.
And the net consensus was it was either one percent or five percent positive. If we now do a phenotype double stain using p sixty three, which identifies the squamous carcinoma cells by positive nuclei, we in fact cannot find a single positive cancer cell. This in fact is a negative result, and and everybody got it wrong, including me on the glass slide.
So we really need a more precise cell identification method, which requires multiplex staining by IHC IHC or IF. This can certainly be done these days. There are many commercial stains out there.
But in my view, this cannot and should not be interpreted manually with the naked eye. It must be done by digital analysis.
Here’s a multiplex, for example, at Curtis the Cliff Hite at Kirken Elmer. The technology has improved considerably in the ten in the seven or eight years since we did this, but it can detect the biomarker shown here in red. We can achieve better cell identification, by phenotyping, immune cells, t cells, b cells, macrophages, and we can count them. And we can get an accurate percentage score by image analysis methods, accurate scoring by percentage, much more accurate than naked eye.
Even then, we haven’t strictly quantified, but we have the potential for quantification if we add this to the fluorescent peptide calibration standards that Steve Bogan has developed, we have the potential for quantification of the amount, comparing intensity versus the reference standard.
We can do that for every marker here. We would require a standard for every different stain in the multiplex. In practice, we may need only to do this with PDL one because it’s the very the variable marker we’re looking at. The remaining cells, we only need to identify. We don’t actually need to quantify the amount of target present.
So this is potentially doable, and this is where the field is moving.
Problem for you as pathologists, of course, is that you can’t read this slide with your beautiful microscope, but this can, namely your computer with whole slide imaging and image analysis.
So what are the problems with digital pathology?
Most of those problems have gone away in the past decade. Not not gone away, but they’ve improved.
Those shown in green have improved dramatically in the past decade. Resolutions now, fantastic. Scanning speed, less than a minute for a whole slide image.
Storage, sharing, viewing through improved transmission, big gigabyte files are easily handled.
Apps are becoming numerous and available and have been validated for quantification, metrics, and analysis.
Hardware costs are still high, but are falling. Software costs are falling because a lot of the software is done by cloud based. You don’t need to keep updating your software.
The two obstacles remain really, acceptance by pathologists and, of course, significant regulatory and reimbursement problems, certainly in the US and also in other countries.
But they’re gradually being approached.
Algorithms, for example, already match or beat pathologists for IHC scoring. This is a study of two hundred and thirty cases of non small cell lung cancer.
Allan Gown, Rim, Huang, and it’s a study in which I participated too. It was looking at lung, two hundred and thirty cases, and the artificial intelligence image analysis algorithm matched or beat the pathologist in this study. And certainly, if you were asked to repeat the scoring, then the consistency of the algorithm, was much better than the consistency or the reproducibility of the pathologist in scoring the same cases. So the methods are there.
It’s a matter of applying them. And there’s nothing new about the concept. It’s interestingly and Arthur Clarke, when he wrote Space Odyssey, came up with HAL as the computer that actually, develops a human like intelligence. And HAL stands for heuristic algorithmic learning, which is exactly what we’re doing today.
And so the resistance to digital pathology and AI, artificial intelligence, the use thereof is is difficult to understand because we use it in our daily life without second thoughts as in Google Maps. So so here I am in Malibu sort of cruising around for half an hour trying to identify and find where all the restaurants are. But I can click and get an answer in a fraction of a second.
There are the restaurants. That’s where they are. And I can look at a tissue section, lymph node looking for micromets, and I can cruise around with my microscope for half an hour and try and count them and distinguish them from macrophages, or I can click on the algorithm and get an answer in a fraction of a second. Tumor cells versus macrophages.
How many are there? Where are they? And this technology in this particular paper is five years old. It’s better today.
And one really interesting set of studies are the chameleon studies that really based on a a Google competition where a number of institutions competed looking at two hundred lymph nodes with metastases to, look for micro mets. Andrew Beck and his group from Beth Israel and the University of Warwick were the two with with the best results. And interestingly, looking at discordance, study pathologists got seven cases amongst the two hundred wrong, three point five percent error.
The AI model was under three percent. But really interesting, if you put AI together with the pathologist, you only missed one case in two hundred, and that probably is where we’re going with this methodology.
So to summarize in one final slide, IHC, today the result is in the eye of the beholder, but with technology, we could make this more objective.
And if we look at just the world we live in, it hasn’t changed in terms of geography very much in the last thousands of years. But our perception of what it looks like has in fact changed dramatically.
If we go here to fifteen forty, here’s the new Novus Orbis, the new world, and this island off the coast of what now is North America. In fact, it’s Japan, and the Pacific Ocean here is just a a short stone’s throw, where in fact that, of course, is wrong, and California really didn’t exist at that point in time. However, as technology and knowledge improved a hundred years later, here’s California, but it’s now an island. And you could, in fact, sail all the way around it up the Sea of Cortez into the Bay of San Francisco and out the other side.
That, of course, again, was a misinterpretation due to lack of knowledge and technology, and it was corrected by the simple expedient of a Franciscan monk walking from Mexico to Mendocino County without getting his feet wet, showing that in fact California was not an island at all. So the technology and the knowledge we have influences our perception, and that should not be true of a diagnostic lab test. And immunohistochemistry is at the stage now where it can be improved and should be improved, and the remaining of this master class series will address some of the issues about what we can and might do.
I include a few references at the end of this presentation that give further detail on a number of the type the topics that I’ve discussed. I thank you for for being with me for this hour, and I look forward to a a q and a session. Thank you.
Thank you, professor Clive, for this excellent presentation.
I would like to invite you now to turn on your camera and your microphone so we can get started with the q and a. And in the meantime, I’m gonna check if we are getting any questions from our audience.
Do you hear me?
Yes. Hello?
Hi. How are you?
Hey. Good morning.
Good morning to you or good evening wherever you are.
Yes. Almost good evening here in Denmark.
So let’s give it some time for people to Of course.
Write some questions. So I encourage everyone, if you have any questions or insights that you’ve got from this presentation, you can write in the chat. I’m gonna read it for Clive and, yeah, we can get it going.
So I can see we have a question from Johanna.
She’s asking, what can we do in the short term to improve quality and consistency of IHC?
Well, I think the the short term, solution is at hand and is sort of being worked on as we speak, actually. I think improving controls is is the key and trying to get agreement amongst different institutions to use at least similar controls. And I think the work of Nordic QC, UKNICAS, the Canadian group, Australia, China, various external quality control organizations are starting to do that. And and there’s no doubt that over the past decade, results and reproducibility have improved by the simple expedience of a lab running a test and submitting the results of that test to some form of central analysis and comparison to see how they stack up against the world at large.
And, obviously, if I’m running a lab and my results when I send them back are worse than other people, then I’ve got a strong motivation to improve that and to look at the issues and the test process in my lab to try to get up to that level. None of us like to be the worst. None of us like to be below average. That’s who we are.
And simply by showing us all what the average is, I think it improves us. So I think that’s the first measure. And if you follow that measure, then the recommended controls are incorporated in the review process. So I think that’s a huge help.
There are a series of articles on controls that I listed at the end of my talk.
Tolokovich is is, Amina is the lead author on most of those, but it’s a large group of people, an ad hoc committee that looked at these issues and made recommendations. I would strongly urge that, you know, anyone wanting to improve their results should pull those papers and look at them. They’re very good.
Thank you. We got another question from Michael. So I’m gonna read that now.
You were highlighting multiplex immunofluorescence for diagnostics.
Will that eventually happen, or will we continue to refine Brightfield?
That’s a that’s a really good question.
You know, we’re so entrenched in in bright field as pathologists because that’s how we train. We train by spending hours looking down a hot microscope, you know, and it’s hard to abandon something that you’ve built your career on. So I don’t think bright field will go away in the near future.
I think for really complex things where we need to look at multiple analytes, fluorescence is currently the winner, because it’s easy to do five plex, six plex by and by Brightfield, you know, we can get to three three plex maybe, but it’s hard to get beyond that with existing technology. There are technologies in the background coming up that will improve that. But, you know, if you do fluorescence and multiplex, you can easily, by AI, convert that fluorescent image into something that looks exactly like a bright field image if you want to see the morphology.
And, you know, that’s been possible now for four or five years.
So I think bright field will persist.
Certainly, where IHC is still used as a stain, it will persist. I think where we’re trying to go to a strict quantitative assay, I think fluorescence on a duplex or triplex may become the dominant method with AI flipping that at a at a touch of a switch as it were to something that looks like straightforward morphology, but also gives quantification.
So that’s a complicated answer to a simple question, but it’s a complicated problem.
Thank you. Emilia, she asked, how do you see IVDR impacting the implementation of digital algorithms in CDX, especially considering that many labs will not have access to digital pathology in the near few in the very near near future?
Well, I yeah. Obviously, as as I mentioned in my talk a number of times, you know, we we’re constrained as pathologists by what we can do.
And, obviously, the environment in different labs is different, different countries is different, and the overall process, nonetheless, does change and move forward. So digital pathology, in my opinion, will become the standard.
I don’t think there’s much doubt about it. I think it’ll become the standard for morphology too, absent IHC, simply because it’s an expert assistant that we, the pathologists, can have to help us with analysis of a tissue section. I mean, the radiologist now, if you go and have a CT scan, they don’t sit there and look at your hundred CT views. They just click and the computer compares it with the previous CT and says, yes. It’s the same or no. This is the difference, and this is where you need to look.
So, you know, what the radiologists do, we as pathologists should be equally smart as the radiologists, right?
So let’s learn from them.
I think it will come. I agree. It’s gonna take time. The regulatory issues are a huge problem in the US and also in other countries.
I mean, getting digital pathology approved for primary diagnosis in the US took one company, I won’t mention their name, I was part of the process as the as the, lead investigator, took about five years and lots of millions of dollars to get that done.
And somehow that log jam needs to get broken so we can all have more ready access for diagnostic purposes. It is a problem, but it’s a solvable problem. It will just take time.
Thank you. And Dylan, he a hundred percent agrees that multiplex calibrated computational approach to PDL one is the ideal, but this would be a different standard than was used in the clinical trials. How would you propose reconciling this?
Well, it’s nice to know somebody agrees with me. Thank you, Dylan.
I’m glad you’re here.
Yeah. How would I propose you do it? Well, you know, I I can’t greatly influence the regulatory process. This is an FDA issue in the US and, similar agencies around the world. So, it at the present time, if you bring out a new device, even a second generation device, you almost have to go through all the same steps that you had to go through before.
And somehow or other we have to short circuit that process. It’s partly a matter of confidence by the regulatory agents that the new methodology, you know, is, as good as or better, and we we need to find a simpler way of doing that. It obviously, to repeat a study that was done back in nineteen ninety seven, nineteen ninety six, comparing Herceptin to the Hercept test. You know, just because we now wanna do it digitally instead of looking down a microscope is absurd, but that’s where we stand currently. And at some point, somebody will figure out that that’s not, that that’s an obstacle and will will will resolve the problem. It’s beyond any of us as individuals.
I personally believe that industry is going to be the driving force for this methodology because it’s such a comprehensive problem that there’s no individual lab. None of us none of our institutions can attack this problem. If you look at the clinical lab, it sits where the immunoassays sat and radio immunoassays sat, fifty years ago when I first started doing clinical pathology. And the problem wasn’t solved by me or any of us. It was solved by Beckman and Coulter, and that’s what’s gonna happen again here.
Thank you. Anu asked, some control tissue can be very difficult to source from surgical tissue. What is your view in using cell lines as alternatives?
Well, I think, cell lines have a lot to be recommended.
You know, some cell lines are now becoming commercially available. Some full tissues, historians, are becoming commercially available.
I personally believe they’re quite good. That the the deficiency of getting a control cell line or tissue from someplace else other than your own lab is that it will have been fixed and processed differently. That is the pre analytic process is different. So at a minimum, if you do that, then you need to, put in a little preanalytic phase to your study just to study your own tissue to show that it is in fact valid for the assay in question. That is, is the analyte you’re looking for still there having been processed in your lab? So I I like control I like cell lines. I like full tissue, but don’t forget that the pre analytic phase can throw your results way off if you don’t also examine that.
Thank you. We have a question from Britt. Is cost of implementing QC in pathology a limitation or it will reduce reruns or misinterpretation enough to be of value add?
Yeah. That’s always a difficult question, isn’t it? Because, interestingly, back in two thousand four when NIST and FDA looked at this, one of their requirements with with for controls was the ideal control was that it should be inexpensive and inexhaustible and widely available. And, obviously, you know, if you go buy a control line or a full tissue from someone else, it costs you money.
Those costs are coming down, but there’s a developmental cost from the companies that make these, and they obviously are are in business to be in business, not solely to serve us.
And so there is a cost. I do believe it improves the reliability of the test. And if you count that in terms of patient days in hospital, rather than having repeat tests, then I think there are huge gains to be made. The problem for most of us is that our hospital administrators, they keep the bucket, they keep the money in different buckets, so they just look at what pathology costs, and they look at what the hospital costs.
And if the hospital’s saving money by less patient days, pathology does not necessarily get credit for that. In fact, it almost never gets credit for that unless you argue at the point with your administrators. So it needs to be a a more comprehensive approach to budgeting. I think it will save money, absolutely, and it will certainly improve patient outcomes.
Thank you. Now a question from Sarah. How do you QA the numerous publicly available or publish published AI image analysis algorithms, or do you recommend using commercial image analysis platforms?
Yeah. That again, that’s another question. You know, good question. We’re we’re really at the infancy with this this field in a sense.
Again, to go back to what the clinical lab was fifty years ago when we were first doing radio immunoassays and immunoassays, these same questions are being asked. How do we cross correlate?
How do we take our own individual lab when we’re making our own antibodies and doing our own labeling and compare that with something that one of the, major companies are selling. The answer really is you have to do an internal validation to show that your methodology that you’ve developed, that you have developed some confidence for in respect to behavior in your environment with your patients.
You need to do a cross correlation study with whatever external system you’re looking at. I do believe that the external systems, the industry derived systems, will, in the long term, turn out to be better simply because they will have a broader correlation than any one of us can actually manage to do it in house. We can’t afford to do it. They can.
Right. Another question from Sarah. Could our organoids in the future be useful as a control increasing the complexity versus cell lines?
Yeah. I’m a believer in in in full tissues.
We published some of this stuff, you know, twenty years ago almost. It’s one of these serendipitous studies where a a clinician at, the Huntington Research Institute in Pasadena, which was was close by where I was working, they’d got a NASA contract to look to see how cells grew in a zero gravity environment. Bizarre, really. But it turns out that when you grow cells in a zero gravity environment or in a rotational process whereby they’re effectively in zero gravity, they aggregate into little steroids very nicely, and you can aggregate two or three different cell lines into a little steroid that, has the complexity and the morphology of a piece of tissue to some extent, and I showed one picture of that.
So I think that that morphologic correlation back with something like HER2 or PDL1, where the surface display is at this point in time important to us as pathologists, has an advantage over a cell line where the cells are simply cytoscentrifuged out onto a glass slide. So, yeah, I I like photissues, but they have the same difficulty in terms of quantifying exactly how much protein is present, as do any cell line. And so they don’t have the calibration potential at this point of the peptide spots that we talked about earlier.
Thank you. I’m gonna read the well, we still have three last questions, and we are almost running out of time. But I’m gonna read this question from Brandy.
Are you able to make recommendation on the poor success rate of immunofluorescence when multiplexed?
In our lab, we can get fluorescence for one target alone, but often when we combined often when combined, they fail.
When we have multiplex and Brightfield, we have success compared comparable to immunofluorescence with only one target. Is there a likely pitfall you can suggest?
Yeah. There’s no doubt that multiplex fluorescence is is difficult. It’s it’s been amply demonstrated that depending on the method you use, you know, whether you strip the previous reagents off or not, which test you do first, you know, which analyte you run first versus second or third, change the sequence, you get different results. So, again, it’s a matter of standardization.
We’ve spent a lot of time, a lot of frustration trying to make this work, and, basically, again, I think the answer here is, the commercial sources, of the companies that are investing, you know, relatively large amounts of money compared with what any of us can do and relatively large amounts of time, produce the better results. So I would recommend you you buy into a system rather than try to invent your own. I think a duplex is fine to invent yourself, but beyond that, I don’t think it’s wise even to try to do it yourself. It’s better to compare the systems that are out there and try to acquire one. And, again, if you’re gonna do it, please do it by digital analysis, if it’s gonna be more than a duplex because the naked eye can’t do this.
Thank you. Maria is asking, how do you see digital pathology in GLP GCP studies? And who should drive the approval? And individual lab cannot drive this alone.
Well, I agree. I don’t think the labs can drive it alone.
Obviously, you know, in in the US, the certification process runs through the College of American Pathologists, the CAP. You have to be CAP certified. There’s a second process called CLEAR, Clinical Lab Improvement Act.
You have to satisfy both of those.
I think CAP cap has done a lot to drive clinical pathology to better standards. It’s been, I think, deficient in anatomic pathology.
One one problem CAP has, and I’ve said this before, is that that they sort of have a conflict because that they’re both setting the guidelines and then they’re testing or certifying each lab for the guidelines that they themselves have set. And I think that it’s wrong to have a a single body both setting the standards and determining whether people are living up to them. So I think that needs to be modified. I think in Europe, some things are better in some ways. So I think the certification bodies need to be brought on board because we all would like to do better.
It costs us money and effort to do better, and sometimes we need somebody to wave a stick over our heads to say do better or else. And I think that’s why we have examinations to become physicians, you know, wave a stick, you know, become a better doctor or get disqualified.
We all need a stick, I’m afraid, but it’s nice to have a carrot too, a better result, and more satisfaction from from what you get.
Yes. So I’m gonna read the last question now from Andrew.
Is it your opinion that ADT’s no longer have a place in the companion companion diagnostic process?
Yeah.
You people have been thinking about questions. So so lab developed tests, I think, in a in an extremely good lab can be very good. I mean, interestingly, Nordic QC did studies on this a decade ago, Soren Nielsen and and their colleagues.
And they were able to show that lab developed tests over a period of three or four years with an external QC program actually did improve and got better across most labs, and in fact, could almost get to the same level as commercially developed, officially approved, FDA approved tests, for example. So lab developed tests can work, but they require extensive validation, and that validation effort is, extensive, and it has to be consistent. You can’t just validate it once and then you’re done. You have to keep doing it.
So I think in the end, lab developed tests, are good to get a test up and running to give you an internal study, but then I think one should try to shift to commercial, approaches as soon as possible, recognizing that that’s gonna be more expensive on a reagent basis. But it will save money, I think, on a your overall test cost.
Thank you. I think that was the last one. So we got I can see in the chat that we received a lot of good feedback on your presentation.
I think I see a lot of comments. Yeah. Wonderful presentation. Thank you. Very informative.
I think I myself learned a lot during this presentation, so I wanna say thank you very much. And, yeah, I think that’s that’s the end. Okay.
Well, thank you all for allowing me into your, offices briefly, and enjoy your master chemistry. It’s, it’s something I’ve enjoyed for years. It will keep getting better with your help, I’m sure.
Yes.
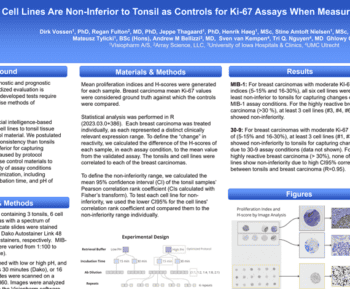
Immunohistochemistry (IHC) entered the realm of Diagnostic Surgical Pathology as more specific type special stain. Today IHC is applied in that role in Anatomic Pathology laboratories worldwide. With the advent of actionable molecular biomarkers, IHC was pressed into service for detection and then quantification of such markers where the IHC result alone could determine therapy. In the latter application IHC was ‘repurposed’ from a stain to an assay. Unfortunately, the necessary pre-analytic, analytic and post-analytic changes did not evolve apace, resulting in poor clinical performance. Key technologies have now evolved to the point that deficits may now be addressed, thereby transmuting of IHC from a stain to an assay – “In Situ Proteomics.”

Clive Taylor, Emeritus Professor at Keck School of Medicine, USA
Dr Clive Taylor is an Emeritus Professor of Pathology at the Keck School of Medicine, University of California. He is a pioneer in immunohistochemical (IHC) techniques for diagnosing surgical pathology, originally adapting these methods in Oxford, England, in 1972. He established a laboratory at the University of Southern California focused on lymphoma research and diagnosis. Dr Taylor has also served as a Trustee and President of the Biological Stain Commission (BSC), collaborating with the FDA to develop guidelines for IHC reagents and enhancing reproducibility.