Transcript
Hello, everybody. Welcome to another master class on the challenges of IHC staining.
My name is Leticia. I work at Visiopharm, and today I’ll be moderating this session.
Our speaker is doctor Steve Bogan.
He’s gonna be discussing the science and the clinical use of IHC calibrators. He’s a clinical otologist. He’s also a professor at Tufts School of Medicine and CEO of Boston Cell Standards. I just wanna remind you all that at the end of this session, there will be a q and a. So I invite everyone to start writing your questions on the chat that at the end, I’ll I’ll read them, and Steve is gonna be following. I hope you enjoy this lecture, and I’ll hand it over to Steve now. And let’s start this webinar.
Hello, everyone. Thank you for joining. I’m Steve Bogan. Before I begin, let me thank the seminar organizers, the wonderful people at Visiopharm, for arranging this immunohistochemistry master class. It’s my honor and privilege to speak with you today about important changes that will affect immunohistochemistry testing. These changes will make it much easier to achieve consistently accurate IHC results.
First, let me explain that I’m a clinical pathologist. Most recently, I served as medical director of the Clinical Chemistry Laboratory at Tufts Medical Center in Boston since two thousand ten. This is my Tufts Medical Center photo when I joined the faculty.
I’m also an NIH funded investigator. The technology I’ll describe was supported by the National Cancer Institute.
Two years ago, I stepped back from serving as medical director to do something new. I now serve as CEO of Boston Cell Standards.
So let’s get started. I mentioned that I’ve directed a clinical chemistry laboratory here at in Boston.
Those tests in the clinical laboratory all generate numbers. For example, a cholesterol of a hundred and fifty five milligrams per deciliter.
In comparison, immunohistochemistry is unique because it generates an image that then must be interpreted.
It makes standardization much harder because we have to compare images.
The important question is whether the image that my lab creates is similar to the image that your lab creates. In this example from Nordic UC, the images from two labs, call them a and b, would lead to different treatments for breast carcinoma even though it’s actually exactly the same tissue.
The fact that the sections are from the exact same paraffin block means that pre analytic issues are identical between the labs. Any differences in the appearance must therefore be due to the stain itself.
Here’s another example, also courtesy of Nordic QC, of substantially different results between, call call them labs a and b, on the same tissue, this time for k I sixty seven.
The problem is that a pathologist working at lab b looking at the image has no way of knowing that their lab’s stain is weak. The coordinators of external quality assessment programs like UKNEQOS or Nordic QC see these striking discrepancies because they see stained slides from all the labs side by side.
Otherwise, there’s no early warning system for an individual lab to quickly indicate to them that there is a problem.
Until now, the answer has been to produce previously diagnosed samples in your paraffin block archive as positive controls.
However, if you’re a lab b and you aren’t aware that you’re a lab b, then using such tissue sections as controls simply continues the problem. We need an objective international standard.
I’d like to show you one more lab AB example, but with a twist.
This is a breast carcinoma core from a tissue microarray stained for estrogen receptor at two different labs, again, we’ll call it a and b, as part of a national proficiency testing survey. Lab a on the left is positive. Lab b, a serosection from the same block, is negative. Again, it has profound implications for patient treatment.
This time, though, I ask you to notice the different lower limits of detection or LODs as indicated under the pictures.
The LOD for lab a is seventy three hundred.
For lab b, it’s seventy five thousand.
This means that an estrogen receptor concentration of seventy three hundred will generate a detectable signal, brown, in lab a stain, while a concentration ten times higher is needed for lab b. Any patient tumors with ER concentrations in between these two figures, between seventy three hundred to seventy five thousand, will be positive at lab a and negative at lab b.
Calibration and its ability to generate and identify the LOD is an early warning system to advise us that we may be insufficiently sensitive.
The image in the last slide was only of the two labs. This graph summarizes the data from all the labs that participated in that published study. Each dot in the graph is a separate labs result. The conclusion is that analytic sensitivity affects whether a tissue section will stain positive, but for a subset of cases. Let me explain.
The graph shows the percentage of positive cases in a breast cancer tissue microarray along the y axis.
And it’s graphed as a function of analytic sensitivity on the x axis as measured by the LOD or lower limit of detection.
At the far left on the x axis, labs have low LODs, and so they’re very sensitive assays. Doesn’t take many molecules of estrogen receptor to generate a visible stain.
The data in this graph are stratified into two groups corresponding to high ER positive cases and low ER positive cases per the CAP ASCO guidelines.
For the high cases, analytic sensitivity doesn’t matter much. Regardless of the LOD, most labs detect approximately the same percentage of positive cases. That’s because the cellular ER concentrations in these tumor cells is so high that even insensitive assays still turn positive.
However, the story is very different for the ER low cases. The determination of positive versus negative is critically dependent on the assay LOD.
Labs with more sensitive tests detect many more cases than those with insensitive assays.
The data demonstrate that analytic sensitivity as measured by the lower limit of detection or LOD directly affects test results and the treatment therefore that patients will receive, but pretty much for the low positive or intermediate level cases.
Therefore, we can use though analytic sensitivity as measured with calibrators as an early warning system for the IHC lab.
I’ve asked colleagues here in the US what they use as an early warning system for IHC testing.
How do you know that your lab is generating accurate images? A common answer is, well, I pass proficiency test surveys.
Yet those surveys show the exact same problem.
These are the proficiency testing data from the College of American Pathologists proficiency testing program for HER2 from two thousand twenty two and the first half of twenty three.
From three surveys, sixty different tissue samples, you see that there’s not a single sample that’s two plus or mid range.
There were samples that some labs scored as two plus, but there wasn’t an eighty percent consensus.
Therefore, those samples were not included in the scoring. In other words, these proficiency tests were unable to simulate the real world situation of two plus or mid range sample.
The severity of the problem led to a series of editorials this year discussing the issue. The editorial second from the top entitled immunohistochemistry should be regulated as an assay is from doctors Magnani and Taylor, where they propose a major overhaul of immunohistochemistry laboratory accreditations in order to address error rates on the order of ten to thirty percent.
The fourth editorial, entitled The Pathologist’s Conundrum, remarked that some tests are no more reproducible than the flip of a coin. The bottom editorial is the most recent and is entitled Immunohistochemistry as an Assay. It was published online just in November. It describes the the endorsement by the National Society of Histo Technologists of the Manani Taylor’s editorial call for regulatory changes. The authors describe the cause of the problem being non standardized controls that are insensitive and irreproducible.
For the remainder of this discussion, I’m going to focus on the call that these editorials have articulated.
That is that immunohistochemistry should be regulated as an assay. So what exactly does that involve?
How would we do that?
How is it different from what we’re doing right now?
I’ll try to convince you that these editorials calling for regulatory reform are right and that we should follow their lead.
To understand what it means, consider the difference in laboratory error rates over the decades. The graph on the left summarizes published reports of error rates in immunohistochemistry where the tests are regulated as stains, not assays.
Each dot is a separate published study of analytic lab errors. The rates over the years consistently remain high.
The graph on the right summarizes published reports on error rates in clinical chemistry.
In that industry, something quite profound happened over the decades, leading to a dramatic decline in clinical chemistry error rates from double digits to less than one percent. Please note the y axis there is a logarithmic scale, underscoring the dramatic decline in error rates. So how did that happen? One of the most important reasons is that laboratory medicine, as a discipline, adopted completely new quality assurance methods. These are the methods when when the editorials describe that immunohistochemistry should be an assay, this is what they’re referring to, adopting the quality assurance systems that clinical chemistry, hematology, microbiology use in the their normal course of day to day testing.
Paraphrasing and condensing the Mignani Taylor editorial, they describe these two critical aspects of laboratory quality assurance that they are missing from immunohistochemistry, but present commonly followed as assays in all the other labs.
The first, calibration, standardizes labs to one another globally. It also aligns clinical labs to any relevant clinical trial assays.
The second bullet, statistical process controls, serve to standardize a laboratory to itself over time. So moving forward, I’ll organize the discussion in this order. First, calibration and then statistical process control.
The concept of calibration is deeply ingrained in laboratory medicine and alluded to in the editorial.
Calibration is foreign to immunohistochemistry.
So I’ll spend just a minute on the concepts.
This ruler can be considered a calibrator, so to speak.
It demarcates a unit of measure length and is traceable to a primary standard.
It comes down to how do I know that this ruler is accurate. It’s not enough to check it against another ruler because that one could also be inaccurate.
Similarly, when we validate an IHC assay against another one, the same situation applies. The other, the predicate IHC assay that we’re comparing it to might also be wrong.
Rather, a manufacturer of rulers checks the accuracy of their ruler manufacturing equipment against a higher order standard. In the US, the highest order standard is at the National Institute of Standards and Technology, or NIST, at the center of this illustration.
The question then arises, okay, how do I know that the ruler at NIST is accurate?
It’s accurate because it in turn is checked against the primary standard at the Bureau of Weights and Measures in France, listed BIPM, shown at the top. So the idea is every the the the ruler in your local hardware store is checked against NIST, and the ruler at NIST is checked against the BIPM primary standard. And how do I know that the BIPM’s primary standard is accurate?
We know because we all agree that these are the units that will follow, and that was that is what makes it a primary standard.
The same concept of measurement traceability to a higher order standard also applies to laboratory assays. In laboratory medicine, there are hundreds of primary standards, typically one for every assay, except, of course, in immunohistochemistry.
The IHC industry lacks any objective reference standards. This is the problem that we set out to solve with funding from the National Cancer Institute, to create reference standards toolkit for every IHC laboratory.
To create an IHC reference standard, we need cells amenable to mass production with defined concentrations of the biomarker we’re measuring. And it has to be low cost, stable, at a homogeneous concentration from cell to cell. So there you see it sort of schematically drawn on the left, an illustration of the patient’s tumor cells with the biomarker we’re looking for as indicated with the red arrow. However, malignant cells don’t really work terribly well for as reference standards.
So we developed the technology to mass produce a cell surrogate, a synthetic cell. As shown on the right, we attached the purified biomarker to a cell sized glass microbead.
Now please take notice of the fluorescein attached to the biomarker.
Typically, there’s one fluorescein per biomarker.
There aren’t any reference standards for any of the biomarkers that we measure in immuno histo chemistry. However, there is a fluorescent standard that was developed at NIST for flow cytometry.
This image illustrates the reference standard, a microbead covalently coated with a fluorescent biomarker, which allows us to precisely measure biomarker concentration traceable to a primary standard at NIST. This system of measurement traceability to a NIST standard ensures reproducible concentration measurements.
These microbeads coated with the purified biomarker behave like cells in IHC tests and have the required features of reference standards.
With tools prepared from these so called synthetic cells, laboratory staff can quickly determine if they are a lab a or a lab b for any particular assay.
The last bullet point is also important.
These standards can be prepared at many different biomarker concentrations.
I’ll explain that on the next slide.
You see here an illustration of how we prepare microbead based reference standards. While synthetic standards probably seem unusual when you first see them, their power is in the ability to inexpensively create any desired IHC biomarker concentration.
It turns IHC into something more like an ELISA.
Typically, you’ll prepare fifteen different concentrations in parallel reaction tubes as shown here, each with a biomarker concentration that is diluted one point six from the next.
From those fifteen concentrations, we select the ten that have the most relevant concentrations for a particular IHC assay.
The high number of data points, now there’s fifteen, then we narrow it down to ten, is actually quite important. If you were to purchase calibrators in clinical chemistry, you’d normally receive five different concentrations.
However, we’ve learned that five is nowhere near enough and that’s because immunohistochemistry amplifies logarithmically, not linearly.
Let me show you.
We’ve analyzed laboratory performance from hundreds of IHC labs, both in North America and Europe. This is a typical example. The data points in orange show the relationship between stain intensity on the y axis as a function of biomarker concentration on the x axis, and that concentration is in the calibrators. Now if this were an immunoassay, there will be a group of data points that line up. You can draw a straight line through them. It’s called the linear range.
Not so in immunosistochemistry.
It turns out that the ramp up in IHC curves is always unusually steep and then flattens out requiring a logarithmic regression line. To adequately define that steep curve and measure the lower limit of detection, you need closely spaced data points. I’ll explain that more in a moment.
It’s also important that each reference standard biomarker concentration is homogeneous.
With chemical synthesis methods, we’re usually seeing a coefficient of variation for each concentration between ten to twenty percent.
In other words, each concentration is distinct from the net from the next one. This graph is a flow cytometric quantification of one of our calibrator series for p fifty three. The data graphically illustrate the distinct calibrator concentrations as measured by fluorescence from the fluorochrome that’s attached to the biomarker. We’ve color coded each level so that you can clearly see it.
Typically, the assay dynamic ranges are between ten to the fourth to ten to the fifth biomarker concentrations or molecules.
Since there are no IHC primary standards, we collaborated with NIST to find a substitute.
Do you remember the illustration of the rulers with the top one at the Bureau of Weights and Measures in France? So this is the equivalent standard which we are using for immunohistochemistry testing.
It’s the description and summary document for NIST standard reference material nineteen thirty four. It’s a fluorescent standard developed for standardizing flow cytometry.
We collaborated with scientists at NIST in creating this system of measurement traceability and applying it to immunohistochemistry.
It now serves as a universal standard for IHC testing. There’s one reference standard for all biomarkers through a link to system of measurement traceability through fluorescein.
This is what the microbeads look like after staining. In this illustration, we just mixed the microbeads with a transformed cell line and stained both of them for estrogen receptor just to illustrate the two side by side. Some microbeads have ER covalently attached to the surface while others don’t, accounting for why some are stained and some are not. It might seem a little odd if this is the first time you’re seeing this, that an IHC calibrator will be a synthetic microbead.
However, there are compelling reasons for their use, many of which are the same reasons that flow cytometry uses similar microbeads as standards. It’s important to keep in mind we’re not trying to simulate the appearance of a cell. Nuclear and cytoplasmic staining are irrelevant for this purpose. Calibrators are for standardizing the analytic portion of the assay.
In assess in essence, we’re turning IHC into an immunoassay so that we can import the same quality assurance systems.
Also, I’ll point out that the biomarker coated microbeads are all formalin fixed. They require antigen retrieval for staining.
IHC calibrators are preprinted on a microscope slide. On this slide, you can see fifteen small round spots, three rows of five. Around the periphery of the spots, there are the numbers one, five, six, and ten to provide you with an orientation to the sequence of increasing biomarker concentrations.
The spot nearest level one has the lowest concentration of calibrator. Ten is the highest. The middle row is comprised of negative controls, which have an antigenically irrelevant biomarker. We provide the exact concentrations for each level on a certificate of analysis. I’m illustrating here how to read a calibrator. It’s actually pretty simple. Identify the lowest concentration level that is still stained.
In panel a above is a schematic representation.
Panel b below are photomicrographs of stained microbeads.
In each, level five is the lowest that still has sufficient color intensity to consider positive.
You’d then look at the certificate of analysis for that calibrator and correlate it with the actual concentration.
Now checking the levels visually is something that anyone can do. In the example here, the actual LOD is likely at a concentration between levels four and five. So to measure it more precisely, we use image analysis.
Image analysis can provide exact quantification of stain intensity at each calibrator level. Like many other assays, IHC analytic response curves are an s shaped or sigmoid curve like this, but with a logarithmic rather than a linear increase.
The analytic response curve defines the relationship of stain intensity on the y axis as a function of biomarker concentration on the x axis.
From the analytic response curve, we can then define two important analytic parameters, the lower limit of detection and the dynamic range. These are the parameters that are your early warning detection system. The lower limit of detection is the lowest biomarker concentration that is clearly distinguishable from the negative control. It’s the biomarker concentration just as the curve angles upward. In this example, the LOD corresponds to where the blue dashed line intersects the x axis. There’s a mathematical formula that I won’t trouble you with right now. As you can see though, an accurate representation of the curve with enough data points is essential.
If you don’t have a sufficiently well defined set of calibrators across the dynamic range of the assay, then it leads to wrong results.
Your early warning system just won’t work.
For this graph to create it, I removed half the calibrators.
The resulting linear regression looks good. The line fits the points, but we know from the previous slide that it’s inaccurate. You’ll end up with the wrong calculated lower limit of detection.
In this situation, a linear regression will push the LOD to the left, much lower than it would otherwise be. You’ll think that your assay is incredibly sensitive when it isn’t. Without a sufficient number of data points to define the curve, particularly across the dynamic range, it’s difficult or impossible to accurately determine analytic sensitivity.
So I’m now transitioning from explaining calibration to explaining statistical process controls, and this part is much shorter.
This graph places IHC controls in the context of calibrators.
This is the analytic response curve that you’ve already seen. An excellent positive control will be one or two calibrator levels with concentrations in the dynamic range. The arrow points to an example.
Now an example of what not to do, which nonetheless is done widely, is denoted in the graph with the red x all the way at the top to the right.
Strongly positive samples are terrible controls. They’re very insensitive.
That’s why you need to know where the control falls on the analytic response curve when you’re selecting one.
Our controls are the same formalin fixed microbeads, but this time as a suspension contained in a vial. There’s no microtome sectioning or retrieving a sample out of the paraffin block archive. You would just take a vial out of the refrigerator. Each vial has enough for a hundred tests.
The laboratory technologist pipettes one microliter of the control onto the slide. After a few minutes, the suspension hardens, retaining the microbeads on the slide. Ideally, the control is on the exact same slide as the sample, namely I on slide controls.
Once the microbeads are on the slide, you handle it exactly as you would for any other for a tissue section. It goes through baking and anagen retrieval and everything.
The standard of laboratory practice and lab medicine is statistical process control, and that’s what you use controls for. In laboratories, it usually takes the form of Levy Jennings charts, which is shown here. It’s for monitoring control values over time to ensure day to day consistency.
Ideally, the data will be consistent over time, and usually it is. With statistical process control, you’re looking for typically one of three patterns.
This is the first one, drift.
Something is slowly changing the instrument or reagents. The pattern offers clues as to the cause. In this instance, it could be a reagent is approaching its end of life.
If it’s an instrument malfunction, it has to be something that’s slowly and progressively failing.
The second pattern is a sporadic outlier. A significant malfunction of some sort has happened requiring repeating the test. Examples include a pump malfunction, a heater failure, drying of the reagent, or a failed dispense.
The third pattern is a worsening of precision or reproducibility.
It can happen in one or both directions with higher and lower QC values as shown here or only, for example, lower.
This might be caused if the pipettor is over or under dispensing or is misaligned, but only sometimes.
It has a random nature behaving in an unpredictable fashion.
In summary, there is a need for better standardization that principally affects patient samples that are in the broad middle of the concentration range. Negative samples, high positives, usually are easy for labs. To solve this challenge, the editorials propose adopting the same quality systems that work for immunoassays, which are calibration and statistical process control.
Calibration aligns lab to each other globally.
Statistical process controls, such as Levy Jennings graphs that I just showed you, they align a lab to itself over time.
Thanks for your interest. I’m happy to answer any questions.
Thanks, Steve, for the excellent presentation. I would like to invite you for the q and a. If you can turn on your camera and your mic so we can get started.
Good. Good. Good afternoon there.
Yes. Good morning to you. How are you?
Good. Thank you. Thank you.
Great. So I’ll give the audience some time to think about the questions, and I’m gonna start myself with one.
So I saw in your presentation that there was a slide that you showed all the editorials that were published recently, claiming that IHC should be regulated as an essay. And I was wondering why this is happening now? What triggered these editorials to happen all at the same time?
Sure.
I I think the reason it’s happening now is because the tools are now available in immunosystem chemistry.
We’ve been working with a number of organizations globally, like Nordic QC, UKNECWAS, CBQA. And so these there are a series of studies that have been coming out.
And I think it just so it’s it’s been a topic of discussion amongst these organizations and many of the leadership in the field, and I I think that’s what triggered it.
Okay. Cool. Thank you.
Alright.
Take a look at the questions.
Don’t be shy, guys.
Okay. I’m gonna read the question from Matt.
So, Steve, how do you ensure beats don’t change in intensity over time? Basically, what is the primary standard for these beats?
So I think if I understand the question, that’s a stability question.
And, what you do is you check stability. We we check stability. So, actually, like, FDA required that. So we formalin fix the controls and calibrator beads, which actually is a remarkable, you know, a way to augment stability. And actually, then we also urge everyone to store the controls in the fridge, and the calibrators actually are frozen.
So the stability goes well beyond the year. Actually, we haven’t found a failure point yet in the calibrators.
Thank you. Sonia is asking how do the pre analytic issues such as formalin fixation relate to the topic?
Sure.
In the three buckets of categories of potential sources of error. There’s the pre analytic as everyone knows, the analytic and the post analytic.
And what we are focusing on is the analytic, and it’s really the exact same like every other part of the clinical laboratory.
There really is no engineered control for pre analytic. In other words, it has to depend on the laboratory and essentially surgery, you know, getting the samples promptly to the pathology lab and getting them into formalin promptly and fixing them for an appropriate amount of time. The is to my knowledge, there is no device that will solve that. And so our any controller calibrator also in clinical chemistry, clinical hematology.
Excuse me.
Bless you.
Yeah. It really doesn’t speak to pre analytic issues.
Thank you. Luis is asking which markers coupled to beads are available?
Excuse me. I’m struggling with a cold, so I apologize for the cough.
No worries. Thank you for joining anyways.
We have the studies so far have focused on the breast cancer panel, HER2ERPR, but there’s a series of others that we have available. I don’t even wanna make this a commercial story.
It’s actually listed on our website, but, and I don’t remember all of them. But current studies I I didn’t mention that there’s there is a consortium that we’re working with. So the current studies in the consortium are PDL one, extracellular domain, p fifty three, BRAF, and, we have k s sixty seven is actually something we have, and we’re just looking at that to get a little better definition on that. There’s a bunch of others which I’m forgetting, but it’ll be listed on our website.
Thank you. Now we have a question from Michael.
How difficult is it to extend the menu of available markers, clones? And do you need different calibrators and controls for different clones of the same biomarker?
That’s a good question. Yeah.
So it’s actually we’ve kind of got it down to a process.
So we actually set up we’re now ISO thirteen forty five certified. So in other words, it’s a like a medic in other words, we’re certified as a medical device manufacturer, and it’s fairly straightforward. It’s the same basic procedure for every single different target. What’s different about it is we have to identify what will we use as the target.
And so in any particular target and, you know, we’re approached for custom targets all the time. And what happens is we have to first decide, are we going to use the intact native protein, which we do sometimes, or are we going to use the peptide epitome? Now addressing the question, if we use the protein, then pretty much the whole protein is represented. So there’s no it’ll it’ll hit.
It’ll be suitable for all the different monoclonals for that protein. If we use peptide epitopes, sometimes we need different peptides. And so it would be specific. So for example, for HER2, all but one of the targets are to the same c terminal peptide.
So the only difference as s p three is to a, an extracellular domain.
So that same peptide works for all the different monoclonals.
But in other instances, like estrogen receptor, they each have their own epitope.
Thank you. Henrik is asking, what do you see as the greatest challenges to getting calibrators and process control running every lab routine, and what are the next steps needed?
Okay. Sure.
Greatest challenges. I I think where we are now, we’re our challenge is we’re working very hard on scaling up, because we’re just preparing actually for product launch.
And we’ve also been working very hard on kind of helping people understand what the upside, what the benefit is in doing this.
Because it’s a big change. This is would be a very large change for everyone. And so the discussions have been at per those editorials, you know, how do we phase this in? I I think it’ll take some time.
I Yes. Yep.
Question from Johanna. How are the new tools used to standardize a lab? And how would someone know the correct lower limit of detection to aim for?
Sure.
So it’s ex they’ll be used really very much like how they’re used in chemistry or immunology or hematology.
But that question, what’s the aim the target to aim for is actually an excellent question.
Because, you know, in other industries, when a new assay was developed and then submitted for regulatory clearance, that question is automatically answered. So in other words, like cholesterol. Okay. We know that anyone with a cholesterol less than two hundred milligrams per deciliter, you know, they might be a candidate for a statin or a TSA, thyroid stimulating hormone. Those are they’re well defined ranges, except not in this industry. It never happened.
So we are working with there’s a consortium that I mentioned for analytic standardization, doing these some of the studies, particularly for the high priority targets, to establish it. Actually, we’re just now getting the data for her too.
And, it look the the consortium steering committee will be meeting soon. We’ll be figuring out that exact question.
Nice. Jeppe has asked, what do you believe has the biggest impact, calibration or statistical process controls?
Hi, Jeppe. I think they go hand in hand.
Calibration, you know, it’s something you’ll do periodically depending on the stability of the assay. So in in the clinical pathology world, we might calibrate anywhere from once a day to once a month, in other words.
For control statistical process control, that really does need to be done every day. So the idea is we align we set up our assay to be aligned with everyone else, and then we monitor it over time every day, day after day to make sure nothing’s changed.
So they go they they you really they’re both needed. And and, again, it’s not me who’s saying that. Just please be aware. It’s not me making this up. This is how it’s used in clinical laboratory medicine.
Alright.
Question from Michael. What argument have you found to be the most compelling to a lab or lab manager in terms of return of investment of introducing a new procedure?
The the initial the laboratories that we’re working with right now, which we’re sort of some of the among the top cancer centers and focused in the US, really, they’re doing it for quality reasons.
Sort of everybody seems to be aware of the challenges and the difficulties in maintaining standard you know, standardized results.
And so we haven’t really invoked the cost argument, you know, the the labor savings argument. However, there’s clearly a a cost argument. It is very labor intensive. It’s an unappreciated cost of preparing one’s own tissue controls, you know, going through the paraffin block archive, identifying them, validating them. So it actually it works out, but that has not been so far the focus of discussion.
Alright.
Juan Carlos, I think you’re asking if these calibrators can be used for cytoplasmic, nuclear, and membrane proteins?
So yes. That’s the question.
Yeah. No. So that and that’s I mentioned it during the lecture.
Everything you know, as the beads are attached to the the the protein or the peptide, the analyte, the biomarker is attached to the surface of the bead. And therefore, the appearance on the bead will be the same regardless of where the analyte was present within the cell.
But really, it makes no difference where the analyte is in the native cell. We just have to identify what form of that analyte we’ll use for the assay.
Okay. Thank you. We have another question from Matt. He’s asking, are these beads stable across all different types of antigen retrieval?
Some methods are very harsh.
Actually, yes. It’s a you know, we, we’ve not we’ve done a lot of imagery, and not just us, actually.
The beads have been used the system, the calibrators have been used probably well beyond a hundred labs by now. I mean, it’s harder.
A hundred and fifty, two hundred. And, they actually sometimes like antigen retrieval. It’s hard. It’s surprising. They the the immunoreactivity generally improves after antigen retrieval, which is not surprising because they’re formalin fixed. And most of the time, formalin fixation, even in tissues, it block hysterically blocks the epitope and prevents binding. So the same chemistry we’ve we’ve I mean, our group actually published the original descriptions of the chemistry for antigen for formalin fixation as it affects immunoactivity.
And, we’ve we’ve replicated that with these calibrators and controls.
Cool. Thank you.
I think that was the last question. Let me double check. I think so.
Oh, wait. I think we have one more from Cindy.
Could you remind me of when you say across all labs exactly how many labs were you part were part of the trial? I know you just said hundreds are using the calibration mode, but how many were part of the study, I guess?
Sure. With the estrogen receptor study, it was about, eighty, of which fifty were using the SP one, but that’s where we focused our data. For HER two, we also have just a little over fifty different labs. I mean, through that was distributed through Equinix plus in Nordic QC. The ER was through in Canada.
PDL one and p fifty three is similar numbers, each one, and, plus just a lot of labs also here in the US that we’ve worked with. So if you add a lot, we’re probably approaching two hundred, I imagine.
Cool. I hope that answers. I think yeah. She commented mainly North America and mainly clinical.
I guess, she’s clinical lab. Right. I mean, the whole purpose was the clinical labs. Yeah.
Okay. Well, thank you, Steve.
Happy to help.
Just one more comment from Sydney. She’s asking if it was mainly breast tumors?
Yes. Most of our work initially has been focused on the breast panel.
Okay. Perfect.
Thank you for the nice presentation and your time. Obviously, especially you being a little bit sick. We appreciate you being here, and thank you the whole audience for joining and engaging with questions. It was it’s always really nice to see. Thanks, Steve, once again, and have a good day, everyone.
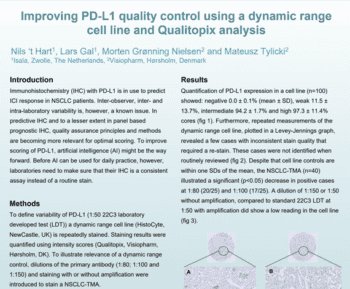
Published studies consistently demonstrate discrepancies in immunohistochemistry (IHC) staining from one laboratory to the next. In practice, clinical IHC laboratories usually report consistent results on samples that are negative or strongly positive. However, tumor samples with biomarker expression levels in the middle, between these two extremes, yield variable results among laboratories. If the IHC test is for a targeted therapeutic, then these are the patients at greatest risk to be treated incorrectly. The answer is to adopt the kind of quality assurance that is used in other parts of the clinical laboratory.
In this seminar, we describe the theory and practice of new IHC quality assurance tools. Calibrators provide, for the first time, a direct readout on the analytic sensitivity of IHC assays. Achieving a target lower limit of detection (LOD) guarantees an appropriate stain intensity. Controls, on the other hand, are well-established in IHC. However, labs are usually not aware if their controls have relevant biomarker concentrations, including whether the biomarker concentration is even in the assay dynamic range. This presentation includes a description of both the science and clinical use of IHC calibrators and linear-range controls, including their objective quantification and use for statistical process control. These more advanced quality assurance tools are required to ensure accuracy and consistency in patient testing.
Steve Bogen, CEO, Boston Cell Standards, USA
Dr Bogen is a Board-Certified Clinical Pathologist, having graduated from the University of Chicago Pritzker School of Medicine (M.D.) and the Weizman Institute of Science (Ph.D.), with a post-graduate residency and research fellowship at the Brigham and Women’s Hospital. He is Adjunct Professor of Pathology and Laboratory Medicine at Tufts University School of Medicine and served as Medical Director, Clinical Chemistry Laboratory at Tufts Medical Center until 2021. He is also an NCI-funded investigator whose research has focused principally on developing better diagnostic tools. Dr. Bogen was previously the founder of CytoLogix Corporation. He now serves as CEO of Boston Cell Standards.