Transcript
Well, thanks everyone for coming. My name is Jenny. I have also with me Dirk today and we’re really excited to talk to you about some of the methods that we’re taking for looking at HER2 low expression and how we can utilize AI to better investigate that group. Just a little disclaimer before we get started, you might see some products that are marked as CE-IVD or IVDR.
Any of those are just for research use only here in the US, so always just like to put that little disclaimer upfront.
As a quick agenda of what we’re gonna talk through today, I’m gonna give just a little bit of background on HER2 Low for anyone that might not be quite as familiar.
We’re also gonna talk a bit about some of the assessment challenges that pathologists have been noting recently in some of the literature. Dirk’s gonna performance history from the past, how it aligns with FISH data, and we have a brand new case study to share with you today as well from a leading hospital.
So just to give some background on HER2 expression, HER2 is overexpressed in about twenty percent of breast cancer cases.
I really like, this picture, this graphic. It kind of displays that HER2 expression is actually a spectrum.
So on the left, you have your, samples that don’t have any IHC expression.
As you move more towards the middle, you have moderate expression. And And then all the way on the right, you have strong HER2 staining expression.
We are looking at HER2 staining because you can effectively target therapies towards tumors that are high expressors of HER2 staining.
Traditionally, those specimens also have, a positive FISH amplification, so they do have that happening with their genes and the overexpression with the IHC staining.
What we actually see is that eighty to eighty five of breast cancer cases are traditionally classified as HER2 negative.
That’s this, red area within the fan here. So all of these patients aren’t eligible for your typical traditional HER2 therapies.
However, within these eighty to eighty five percent of cases, we actually see that about sixty percent do have this low amount of HER2 expression.
We’re really focused on this HER2 low group because this is another subset of patients that we could have targeted therapies for, especially as we’re starting to see some FDA approved therapies specific to HER2 low coming through.
There’s a recent publication I’ve got down here at the bottom for you, but, I really enjoyed reading through this because it brings up some of the reasons that pathologists are questioning the HER2 low subgroup and being able to identify those cases.
It’s a little bit of a twofold approach.
First, they are talking through if the IHC assays are optimized and reliable enough to properly assess HER2 low expression levels and also how you can address pre analytical factors that could possibly impact your IHC staining, which would then ultimately impact possible interpretation.
On the other side, they’re also questioning reproducibility between readers and daily practice and if the traditional HER2 scoring method is the right approach for looking at these HER2 low subgroups.
What we’ve been working on at Visiopharm is really to address this with a two pronged approach.
So we are working with Qualitopix to identify staining consistency needs and also an AI, HER2 algorithm in our Oncotopix platform. And I’ll let Dirk speak a little bit more to those and take you through some of the Qualitopix work.
Yeah. Thank you, Jenny.
Yeah. So on the left is a is a solution that we have developed, which is really focusing on measuring and and giving some information on the on the stain, the quality of the stain itself. This works for a couple of assays, including HER2, but we also have PD L1, and very soon ERPR and KI67 will be out as well.
It basically helps a lab to determine how the staining consistency is. So a slide coming out of the lab stained with one of these assays, how does that staining quality relate to yesterday or the week before or last month? So it’s that variation that we’re measuring. So that’s a tool really looking at the inputs that goes to the pathologists, actually the output of the lab.
Then on the other side, we have apps that assist pathologists in decision support, so quantifying these assays, so counting, but also determining, which areas are are the right ones to analyze. The apps have been on the market for a long time. Traditionally, these apps would require pathologists to outline, the region, typically the tumor region for for analysis.
Then the pathologist could go and drink a cup of coffee or tea and then come back and review the results. We are now taking that to a really next level. We have a pipeline of apps where a tissue a digital slide comes in, then the quality of the tissue is is identified. The region to be analyzed is identified.
Basically, where is the tumor, where is the relevant area of the tumor, and then within that region, the cells are detected and quantified.
So basically, at the first time that the pathologist sees these assays, everything is available for review and the pathologist basically needs to QC and see if if they agree with what the app came up with. So let me give some more information on Qualitotics, and then after that, I’ll hand back to to Jenny to talk about the HER2 app that the pathologist would would use during the review of the slides. But this is, again, looking at the variation of staining coming from the lab. We all know probably that that there is quite a bit of variation introduced in the lab in the staining itself. How the biopsy is taken, how the sample is treated, how the slide is made, how the staining is done, all kind of variation that adds up before it even gets to the pathologist. We are focusing on a very specific area here. So not all of this, not this whole stack, but we are focusing on how reproducible is the staining itself.
And that is a problem that that is significant, and we have data from EQAs, and I reference here a paper from Nordic UC, where about twenty to thirty percent of all assays that they review, that they are actually insufficiently stained.
So that’s not visual form data, but that’s independent data. And that, of course, has impact on patient outcome potentially, and then, of course, also the cost to the health care system.
So basically, the approach that we take is that to the sample that is stained, on that slide, there is some reference material added that can be cell lines. We have started with cell lines, but it could also be microbeads or other standardized reference materials. And they’re standardized because these materials, they have a known level of expression of a certain protein.
So you know what it should be. You know the ground truth, so so to say. These cell lines, in this case, they’re added to the to the slides when it’s stained, then it’s digitized, and then it’s uploaded to our Qualitopix platform. It’s a cloud platform, and their apps analyze that that slide.
These are two examples on the left of insufficient staining and on the right of sufficient staining. And these are from data that we have collected from from a trial that we have done and I’ll talk in more detail about that, but you see kind of the difference. Same sample but different staining results. So one thing that we do is we collaborate with EQAs. They’re kind of the experts in the field on on what good staining looks like. They help labs with identifying the quality of the stain, but they also help labs with with troubleshooting if there are issues with with staining.
And this is data from UKNECROS where actually four labs are plotted over time how they do with their staining quality. So you see that there are labs who are good over a stable period, there are labs who are not so good over a stable period, but there are also labs that are good, then lose it, and then find it back again. So there is a whole range of behavior.
And I think this is known, and the EQA is published on this. But the question that we asked ourselves is, what happens actually between those EQA runs?
Right? This only happens every six to twelve months, sometimes even with a lower frequency, but what happens on a day to day variation or a sample to sample variation? I think I already explained a little bit why we use cell lines, but it’s important to to spend some time on that. Basically, we need something that is stained where we know how it should look like.
So you need some standardized reference material. Typically, these cell lines have three, four, five cores, typically a low and a high expression level and then also two levels in between to get a quantitative result. The cell lines there are provided by external vendors. Visiopharm is really not in the business of cell lines, and we work with with the good companies that are out there.
This is some of the results. We have now tested with more than twenty labs this approach, and there are some really interesting results.
But basically, the platform allows a lab to track the staining variation over time. So if this is what you see today, how does that compare with what you saw last week or two weeks ago?
When there’s a significant change, when it goes outside of range, then the platform notifies the lab. So you can go in, you can take a look like, hey, what’s going on? And then also look at the images and troubleshoot your process.
On the right, there are some examples. On the on the top, the graph shows how kind of a stable lab works. So all the curves are pretty flat, not exactly flat, but they’re relatively flat. In the second curve, you see an example where a lab first used a certain clone and they had really big fluctuations, and then they switched to to another clone, and they saw the variation being reduced. And then on the in the final graph, you see on the left, you see a bump in the data where it’s kind of started to drift.
And then when the lab started to look into that and and troubleshoot, they found that they had a issue with the protocol, which they didn’t realize. So when they fixed that, the results became stable. And on the right in that graph, you see that they detected some instrumentation issues. And when that stainer instrument was fixed, again, the curves became flat.
The workflow is super simple. We have really designed it to make it very simple to adopt. So basically, a lab purchases some cell materials. Those are those blocks are cut and put on the on on a slide.
Could be with every patient sample, could be once a day, could be once a week. We see a variation of that. Some labs use it every for every sample, some others at a lower frequency. Slides are are stained. They’re scanned and then uploaded, and that’s basically a drag and drop, super simple, takes less than three minutes and the results are calculated and the lab basically gets the feedback on what’s happening.
We have really designed this in the most low friction way we could think about it. So there is no LIS or PACS integration needed.
There is, no PHI being uploaded. These are cell lines. And then it’s super simple and fits in the in the with HystoTech workflow.
So we want this to to work for for every lab that has access to a scanner. You do you don’t need to be fully digital. You don’t need to be on the road to be fully digital. If you have a scanner somewhere and you can scan a sample, then then you’re good to go. With that, I’m gonna hand back to Jenny, and we’ll continue with, HER2LO.
So what DIRPS really addressed is how we are meeting those pathologist questions about making sure that they have consistency and sensitivity to their staining assays upfront. So once we’re able to measure that and make sure we have that consistency, then we can move into the image analysis phase where we really start to look into how this could be a tool for the pathologist during their interpretation and assessment.
So within our Oncotopix platform, we have an AI driven HER2 app, really again for the assessment support for the pathologist.
This was actually the first IVDR certified AI in the entire world. Again, research is only here in the US.
It will automatically calculate the HER2 score in line with the ASCO cap guidelines. And And it also has a proven track record of identifying IHC positive but fish negative cases and this is a big part of that HER2 low subgroup. So we’re gonna talk a little bit more about that data and some real world data that we’ve gathered with that too.
We also have a semi automatic workflow and we’re always working towards that fully automatic workflow. So we’ll give you a sneak peek of how those are looking as well. When I say we have the semi and the fully automated approach, really this speaks to how are we identifying the tissue and those tumor regions for for the analysis to run within so that it’s prepopulated as Dirk mentioned for the pathologist when they go to do the review.
So what you’re seeing here is an example of that semi automated approach. So the pathologist will go in with our annotation tools and they will circle the area that they feel is appropriate for the HER2 assessment.
Alternatively, we’re working towards fully automated solutions, and this really starts at the full slide level. It allows us to do analysis within the whole tissue and even starts at the point at automatically distinguishing on-site controls versus your patient tissue. Really, what we’re trying to do is remove any steps where the pathologist or a technician might have to go in and remove anything that’s not of interest or circle the tissue itself.
After that automatic tissue detection, the AI algorithm goes in and it will automatically identify tumor regions.
It will also delineate them between invasive versus non invasive regions such as DCIS.
As part of our studies towards this, we’ll be looking more into what the performance of that looks like for things like properly ignoring DCIS and identifying tumor.
Within those invasive tumor nest regions, then the HER2 algorithm runs, and that’s going to produce that traditional HER2 score.
Really, the algorithm works by identifying DAB positive membrane structures on the tumor cells.
So it really looks at a combination of the connectivity of the membranes, the size, the distribution, the intensity.
Really, it’s asking, do you have this kind of chicken wire mesh pattern that might be more indicative of a three plus sample or is it more fragmented like a one plus or a two plus sample might be?
Again, you’ll have that traditional zero to three plus HER2 output score, but we also produce a continuous score that is a zero to one connectivity score as a secondary data point.
One of the questions that the pathologists have been bringing up in the literature is if the traditional HER2 score is the right endpoint or if they should also be looking at secondary endpoints.
So we’re really investigating the connectivity score.
There are other scoring breakdowns that we can do and that we’re always working with some of our partners and pilots to further investigate.
So this right here is an example where we have further broken down the membrane classification into to really a a low, medium, and a high connectivity. So you’re seeing in blue there the lower connectivity. Then as you get closer to that red or that pink, the higher levels of connectivity.
So again, just different exploratory endpoints that we can use with the AI toolbox to have secondary data points for the pathologist beyond the HER2 score.
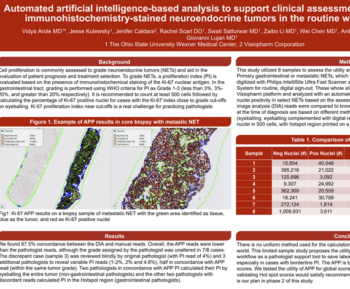
I know there’s a lot on this slide, but these are two publications that I always enjoy sharing. These are just some of the proven track records of the HER2 app and how it relates back to manual reads and to fish.
So on the left here, you have a study done by, the group at Ohio State, doctor Parwani’s lab, where they looked at six hundred and twelve breast cancer specimens. So those were IHC stained, digitized, analyzed using our HER2 algorithm, and FISH testing was also performed on those.
So what you’re seeing in this top graph is the Pearson correlation coefficient for the HER2 connectivity score that I mentioned compared back to the HER2 fish copy number and that correlation is about point eight six. We tend to consider something over point seven to be well correlated.
The lower graph is the same measurement, but it’s comparing the connectivity score back to the HER2 fish ratio instead of just the HER2 copy number.
On the right, we have a secondary study from a European lab.
Again, they ran our HER2 algorithm, but this time we’re looking a little bit more into how that matches with some of the pathologist manual reads.
So what we saw is that at the spot level, which were smaller regions placed on the tissue, you had a kappa score of point eight six and within the full read of the tissue of point eight seven.
I really enjoyed this quote that’s the third bullet point here, which was that they felt the most immediate benefit of integrating the digital algorithm into the routine workflow is that it could alert or reassure the pathologist of potentially misinterpreted IHC zero or one plus versus two plus cases, kind of as that quality checkpoint for them or that second set of eyes.
It also provided them, again, that continuous variable reflecting HER2 two IHC expression, which they also found useful for quality assurance.
We’ve also been running a pilot recently and we have this brand new case study to share with you from Massachusetts General Hospital. So special thanks to doctor Joe Massachusetts General Hospital. So special thanks to doctor Joe Leonertz and Eula Green for working with us on this pilot and allowing us to share this data with you today.
In this pilot, we worked with fifty eight patient samples.
These samples came from five different hospitals within the system. They were also variably stained with two different HER2 antibodies and each hospital had their own kind of upstream workflow of how they process and how they stain these specimen.
Once these slides made it over to Massachusetts General Hospital, they were annotated on the glass slide by a pathologist.
They were also digitized and then fish testing was performed.
Once we had those digitized images, we tested out both the semi automated and the fully automated workflow with our HER2 algorithm.
So for the first workflow, we were able to utilize the pathologist inking on the glass slide to manually denote where the analysis should be ran.
In the other workflow, we did the fully automated method, so detecting the patient tissue, the tumor automatically, the invasive tumor, and running the HER2 within that.
I think Dirk phrased it well when the idea is that we really want to automate this as much as possible so that you’re able to step away, you’re able to grab a cup of coffee. In this case, we set up these analyses one evening, came in the next morning, and had all the results ready to review. Again, just always working towards that automated process.
So I’m gonna walk you through some of the performance results.
Within these grids, what you’re seeing across the top is the IHC manual assessment at sign out. What you’re seeing, diagonally I’m sorry. Straight up and down are going to be the image analysis scores. So we have the fully automated workflow and the semi automated workflow.
So any box that’s labeled green, that’s going to be concordant. So So any box that’s labeled green, that’s going to be concordant. So where the image analysis HER2 score match that of the pathologist, anything yellow is going to be a minor discordance. So maybe the image analysis called it a three, the manual score called it a two, but ultimately, it doesn’t necessarily change the treatment strategy that the team might make.
In red, you’re going to see a major discordance. So anything that would change the patient treatment strategy, those are labeled in red.
We also have this blue box. So these blue boxes are a discordance.
It’s where the pathologist called a specimen a two plus for IHC, but the Visioform algorithm actually called it a one plus. So these could potentially have a positive impact for the discordance because these have the potential to be some HER2 low specimen expressing IHC staining but FISH negative.
Because MGH did also perform the FISH testing on these samples, we were able to dive into those blue box cases.
And in those cases, they were FISH negative. So the algorithm did properly identify them as a one plus case, meaning they have low HER2 expression but no fish positivity.
So just to go over some high points of this data because I’m sure you all have a few questions in your mind.
Respectively, nineteen and twenty two cases were appropriately reassigned by the HER2 app using both the fully and semi automated workflows.
Labeling those cases with the new HER2 score that differs from the manual score that was given at sign out, again, could be a flag for the pathologist to go in and do an additional examination. They can confirm that proper classification, and just be that final quality checkpoint. I’m also sure your eyes are jumping to this, one case here in the red box. So this was a one plus score manually by the pathologist and a three plus score by the Visiopharm AI app.
You’ll also notice that this only occurred in the fully automated workflow and not in the semi automated workflow. So when we pulled up the specimen and we took a look, we actually found that there was black excision ink on the edges of the tissue. And in the fully automated workflow, the algorithm was actually picking up this excision ink as positive dab membrane staining. So in color space, you start to get really close between black and brown as that brown gets really dark.
So there’s a few ways we could address this.
One way is by using the semi automated workflow or having the pathologist give that final input so they make sure that that excision ink is excluded.
But we’re an AI company and so this is great training data for us to use to further train our algorithm so that it can exclude Excision Inc. In the future. One more artifact that we can automatically exclude.
We also found it really interesting that the AI didn’t seem to be influenced by the hospital’s use of different clones.
So we know when we developed these algorithms, we tried to include some of that upstream variation to have a really robust app. So that includes things like different antibodies, different clones, utilizing samples from different labs that you capture a lot of that in the training data upfront.
We also didn’t see any trends, between which hospital produced specimen that tended to be concordant, discordant, or specimen that were now pulled into that one plus category with the AI.
We were kind of curious if trends like that might emerge between the hospitals, but we didn’t quite see any of those.
So we’re just gonna give a quick summary here. I think I’ll let Dirk take this one over and then make sure that we leave some time as well to answer some questions that you all might have.
The summary is really, really quick. I think with Qualitopix, we have developed a platform that together with reference materials allows a lab to get feedback on the understanding consistency.
Right now, it’s that and not more, but we’re aiming to develop further and really also have the inter lab variability.
And there are some more things on the road map that we think we can take this towards. But for now, we’re already super excited that we have a tool that, that gives a lab feedback on how the staining went.
So really what what we wanted to summarize is the labeling of cases with a HER2 score that differs from what the pathologist initially give was given at sign out. They’re just an example of a case that could be flagged for additional examination by the pathologist so the pathologist can confirm the proper classification.
They They can go back, they can take another look at those fish results or if they want a secondary set of eyes from another pathologist, this is simply a quality control checkpoint and a flag for them in that way.
We also recognize that any discordant samples can always be addressed by the observer. The pathologist always has the final say. The pathologist has the final eyes.
So we know that the AI is always a tool to be used in conjunction with the pathologist.
You can always make that final adjustment. You can always override that score. And some of these studies, such as the Excision Inc, confirm that to us while we’re still training some of the tools.
Good.
Alright. Well, thank you again, everyone.
Thanks a lot.
Dive into the world of HER2 expression with Visiopharm’s Chief Diagnostics Officer, Dirk Vossen and Technical Sales Specialist, Jeni Caldara. They’ll be showcasing our innovative two-step solution for interpretation. Confirm your HER2 staining consistency for accurate assessment, and use the vendor agnostic HER2Connect™ app for scoring interpretation. HER2Connect™ has a proven track-record in identifying HER2-low status specimens, a traditionally challenging group to identify through manual interpretation. Don’t miss this opportunity to improve your HER2 interpretation process.
-
- Investigate staining proficiency and discover the only commercial AI technology available to monitor HER2 staining consistency continuously
-
- Learn about our IVDR-certified HER2 Breast Cancer APP and see real-world performance data produced at a leading US hospital during a research study
-
- Discover how AI-powered decision support can aid in identifying HER2-low specimens

Dirk Vossen, Chief Diagnostics Officer, Visiopharm
Dirk Vossen, leads a team to develop diagnostic and clinical applications of digital pathology. He has a strong track record of creating value through innovation in digital and computational pathology, covering the full range of development from ideation to validation and certification of medical devices and commercialization strategies. With over a decade of experience as a global leader in building digital pathology solutions, Dirk has expertise in developing whole slide image scanners, image management systems, computational pathology applications, and executing clinical programs. He holds a Ph.D. from the AMOLF Institute and Utrecht University.
Jeni Caldara, Technical Sales Specialist, Visiopharm
Jeni Caldara is an innovative digital pathology professional with 6 years of experience in AI-based image analysis and workflow implementation. With a background in cell biology, she brings creativity to the generation of AI solutions that highlight tissue-specific processes. As a Technical Sales Specialist at Visiopharm, Jeni is based in the Colorado office, where she focuses on translating product offerings and integrating them into existing systems at customer sites.