Transcript
Welcome to the webinar on impaired dendritic cell homing in COVID-19.
I welcome you from the Institute for Pathology and Molecular Diagnostics at the University Hospital in Augsburg, Germany.
My name is Ralf Hus. I’m a professor of pathology at the Institute of Pathology and Molecular Diagnostics, and at the same time, deputy director and professor at the Centre and Institute of Digital Medicine, also in Augsburg.
The Institute of Pathology is part of the large regional and university hospital in Augsburg, serving more than two million people in the region.
This, of course, also implies the medical care for those patients who have been infected by COVID-19, pandemia and associated diseases.
One of our main focus over the past two years of the COVID-19 pandemic was the performance of autopsies to better understand the disease and the consequences for the progression of the disease and potential treatment opportunities.
In this map, you see all autopsies performed in Germany, as you can also see that Augsburg was the second largest centers performing such autopsies.
Only Hamburg performed more autopsies, but most of them were of forensic origin and with a different focus than what the Institute of Pathology has done here in Augsburg.
During the first wave, including the variants alpha and beta, nitron autopsies were performed on twenty two COVID associated death, which resulted in several publications on such autopsies.
Here is just a selection of some of those publications dealing with the way autopsies should be performed in a highly contagious disease, which is associated with a very high mortality.
Some studies also included the mapping of the viral load throughout the body, and of course, with particular focus on the presence of the virus and virus strains in lung and the upper airways.
Today, my colleague, Lucas Beuscherding, after my introduction, will present his data on impaired dendritic cell homing in COVID-19 lungs.
Let’s try to understand why this is so important.
COVID-19 predominantly affects the lung tissue of infected patients And during this infection, it causes a diffuse alveolar damage in different stages.
And most of the viral RNA was detectable in the upper airways and lungs, while there are also other parts of the body where wild DNA could be detected, but at a certainly lower frequency and tighter.
As mentioned before, there are three clinical stages of diffuse alveolar damage associated with COVID-19.
The first stage is the so called exudative diffuse alveolar damage, which causes a thickening of the membranes and also a thickening of the alveolar walls, which will decrease the exchange of oxygen between the airways and the blood.
During the second clinical stage of DAD called organizing DAD, a proliferation of fibroblasts starts to continue the thickening of the alveolar walls and also stiffening more the entire architecture of the lung.
The end stage DAD continues with the increasing solidification of the lung tissue with more collagenous fibrosis and very stiff lung tissue, which almost completely help us the exchange of oxygen.
Of course, the clinical surveillance and critical care of those patients increasing during the different stages of the disease, requiring more intensive care and also extra membranous oxygenation of the blood.
We also looked into some possible explanations of the immune response in the different stages of COVID-19 DAD, and came along a publication by Nienholt et al, who described two distinct immunopathological profiles in lung autopsies of COVID-19.
One population showing high interfere levels, while others seem to have lower interference.
Why is this so important?
Interference is a critical player in the maturation and activation of certain cellular immune components.
It is involved in the maturation and homing of dendritic cells, along with the presentation of tumor and viral antigens, and also the activation of and homing of antiviral T cells, and also the selection of antibodies generated by activated B cells.
Only if this entire cellular portfolio does exist at a functional level and a significant number, a viral infection can be coped with, and a patient has a chance to survive the disease.
Along those lines, there have been other publications explaining the role of COVID-19 and associated viruses in the immune response.
It was shown that the upregulation and presentation of viral antigens could be impaired due to a lack of MHC class one or two upregulation.
And SARS-CoV can also be able to infect monocytic derived dendritic cells, which interferes with the functional presentation of antigens to allow an activation of T cells.
At the same time, Saskoph Zweig also changes the expression of certain chemokines, which might alter the homing of dendritic cells to the affected organs.
Simultaneously, there are data pointing towards an impaired maturation of dendritic cells.
So many questions remain even after two years of COVID-19 pandemic.
It is still a question on the role of immature dendritic cells, on their maturation and their possibility to reprocess antigens, whether the recruiting and activation of immature dendritic cells is hampered due to virus infection, whether activation, including the presence of danger signals, is still present, and other mechanisms that involve the maturation of dendritic cells and an adequate cell mediated immune response.
One of the aspects of the immune response, with particular focus on the role of dendritic cells in diffuse alveolar damage, will be presented by my colleague and student at the Institute, Lukas Beuschading.
Thanks a lot for the introduction, professor Hoos.
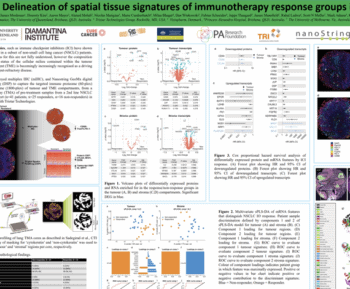
Alright. Let’s get to our brief research report, impaired dendritic cell homing in COVID-19, which was published in Frontiers in Medicine Pathology in November twenty twenty one.
My name is Lucas. I’m in the last year of medical school in the Technical University of Munich, and I paused in twenty twenty for a year to do a bit of research in Augsburg.
What we wanted to do was take a look at the inflammatory infiltrate in the lungs of fatal COVID-19 cases.
In this particular study, we examined the lung tissue of the COVID-19 autopsies of the first wave in Augsburg.
At that time there was a huge amount of papers on COVID-19 getting published and some of these focused on the immune dysregulation.
However, we found that most of these works were about the peripheral blood count So there were actually very few studies taking a look at what one might call the most commonly affected organ in COVID-19, which is the lung.
Now there were a few works using conventional immunohistochemistry autopsy tissue and some using bronco albulaavage fluid but not really detailed descriptions of the local inflammatory infiltrate.
As mentioned before coronaviridae have been reported to affect dendritic cells so we decided to investigate the population of antigen presenting cells.
In the first wave in Augsburg, nineteen COVID autopsies were performed out of twenty two COVID-19 deaths in the university hospital in total.
We are still very grateful to the relatives of the deceased to agree to the autopsies during these trying times. Now some cases underwent only partial autopsies, which is why we started with eighty three lung lobes.
All of these cases were first stained with conventional immunohistochemistry on CD4 and CD8. There was a very scar CD8 reaction, by the way.
And the lobes that didn’t show an adequate reaction to the stains were discarded.
We then constructed a tissue microarray of the remaining eighty one lobes, ten cores per lobe, and proceeded with the immunofluorescent staining.
Some showed processing artifacts and were also discarded.
Out of originally eight ten cores, six zero eight were stained satisfactorily in the end.
These remaining lung lobes had already been analyzed for a different study and assigned a diffuse alveolar damage stage.
So in the end, we had six hundred and eight cores from seventy one lung lobes from seventeen patients.
Unfortunately, there was not a large number of stage three lobes or end stage DAD and also not a large number of non DAD lung lobes.
The stain we used was the Ultimapper fixed view APC kit used to stain antigen presenting cells.
So we had CD24 b cells on the FITC channel, CD11c for myeloid dendritic cells on Cy5, MHC class two on Cy7, and a cocktail of CD68 and CD163 tumor tissue macrophages on Texas red.
The way this works is that after staining each fluorophore gets scanned sequentially so the end result is one insanely large image file containing five layers.
The fifth layer being DAPI to stain DNA.
That means that every single cell in theory can take sixteen different states.
However, of course, not all of these states are biologically possible.
Stay with me just a little longer and we will get to the pretty pictures in a minute.
If you’re dealing with this amount of multi dimensional data there’s no way around digital image analysis.
For this project the multiplex phenotyping module by Visiopharm was the ideal method.
To put it simply the first thing the software does is scanning for the DAPI signal.
This process is based on deep learning. If there’s a somewhat round structure with a certain intensity of DAPI, it gets marked as a nucleus.
Again, this is a simplification.
Next, for every single cell the intensity of each channel is evaluated.
You can also adjust the settings for example if you have a rather strong background signal in one channel.
Now the module automatically generates a list of all detected cell types based on the surface antigen expression.
For example, there are cells expressing CD twenty only but also cells expressing CD twenty and MHC class two as well.
Additionally, Visiopharm also lets you generate various graphs such as phenotype plots, interactive t SNE plots, etcetera.
And while we are at it, I would also like to thank Alima Texan from Visiopharm again for her excellent support and for her endless patience.
Here’s an example of the user interface in Visiopharm.
On the top left, you can see what it looks like if all channels are activated.
As you can see there are four cells and one of these is very brightly stained.
The top right shows what it looks like when only the DAPI and CD11C channel are activated.
On the bottom left, MHC class two and DAPI.
And finally, in the bottom right is Visiopharm’s interpretation of the cells.
Three of these cells were assigned the class negative and marked in gray, and one was assigned the class MHC2 positive and CD11C positive and marked in bright orange.
Now at this point it might still seem like something that could be done manually if you’re very very very patient.
But if you look at what you’re actually going to work with it becomes a bit overwhelming very quickly.
And this is Visiopharm’s interpretation of the image.
MHC class two only positive cells are marked in pink. They are mostly epithelial cells in this case.
We have negative cells in gray, macrophages marked in red, and drum roll, one dendritic cell marked in orange.
Right here.
Now this is a prime example of a cell that would have certainly escaped my attention.
After the classification, Visiopharm can also be used to automatically count the cell populations.
What we have here is the fraction of cells in a certain category divided by the total cell count.
As you can see, we didn’t include end stage DAD lobes in the analysis due to the low count of only three samples.
The b cell count and the macrophage count didn’t show any significant differences, but there was an increased count of myeloid dendritic cells in stage two compared to stage one.
Interestingly, there was no significant difference in the MHC class two expression by MDC in the different stages.
This is remarkable because of the viral mapping paper by Hirschbuhl there was an inverse correlation of viral load and DAD stage.
So we took a closer look to see if there was a correlation of the MHC class two expression by MDC and the detection of viral RNA in the samples, and we didn’t find one.
As mentioned by professor Huss before, in the process of DC maturation, there’s a shift in the surface antigen expression.
Now activated DC show an up regulation of MHC molecules as well as co stimulatory molecules like CD80, CD86, and CD83.
So these markers can be considered maturation markers.
If DC failed to up regulate these markers, this might be a sign of a defective maturation process.
So we attempted further stains of maturation markers, this time using conventional immunohistochemistry.
The problem is that these maturation markers are not particularly specific for DC.
They’re also harder to analyze.
Here you can see a double stain with CD83 marked by Fastred and CD11 c marked by DAB.
As someone who more or less learned to do AI analysis before classical IHC analysis, I was kind of surprised by how ambiguous these stains can be.
The arrow is pointing to a relatively easy to distinguish double positive cell, but not all double positive cells were as good to see.
Now, once again, here’s the comparison to the multiplex stings where you can just switch off the display of certain channels if needed.
And there’s also one more problem with conventional IHC.
For me, it meant having to count the cells manually.
So analyzing the conventional stains means sitting in front of the microscope or the bright field scans for several days and basically click a train yourself.
While this process is a very repetitive task, it is also highly subjective and error prone.
In the end, the IHC stains in general confirmed our findings, but due to the varying specificity, these results should be taken with a grain of salt.
If you’re interested in further details, there’s a link to the paper at the end of the presentation.
Let’s recap. We compared the population of antigen presenting cells in different stages of diffuse alveolar damage in COVID-19 lungs.
There were no significant differences in the count of b cells and macrophages, but an increased count of MDC and later DAD stages.
There also was no correlation of viral load and MHC class two expression in MDC.
At the same time, previous works have established an inverse correlation of DAD stages and viral load.
We also stained the lungs for co stimulatory molecules using them as DC maturation markers, none of which showed a higher expression in early d a d stages.
What could this mean?
In later DAD stages, dendritic cells appear to accumulate.
There is no significant upregulation of MHC class two molecules and other maturation markers in early stages.
This could indicate a generally hindered MDC maturation process.
As the shift in surface antigen expression is what enables MDC to leave the site of acute inflammation and home to lymph nodes, this disruption of the maturation process might ultimately lead to an inadequate activation of T lymphocytes.
There are still a few open questions and some limitations to the study.
The first problem is that the case number was rather small, and also we couldn’t investigate lungs of corona variants.
I also don’t feel completely comfortable making statements about non DAD lungs, And, of course, nonfatal cases would also be interesting to observe, but taking lung lung samples, tissue samples from ARDS patients with a known cause is hardly to justify.
I also want to point out that the actual cellular mechanism is still unclear. So far, it’s just a theory.
So as always, further research needs to be conducted.
If you want to fully understand our work, I suggest you read the original paper as a webinar of course sometimes requires a few cuts regarding the content.
To read the full paper, please follow the QR code using the camera of your phone or just use the DOI link.
That’s it. Thank you for your attention and feel free to send any questions to the email address below.
Thank you.
The high mortality rate of COVID-19 is largely due to acute respiratory distress syndrome (ARDS), which is characterized by diffuse alveolar damage (DAD). Additionally, severe cases of COVID-19 often result in a cytokine storm and a disrupted adaptive immune response. Most previous studies on this issue have focused on the peripheral cell count and the functionality of immune cells.
The team at UK Augsburg in Germany used multiplexed immunofluorescence to study the impact of SARS-CoV-2 on antigen-presenting cells. Like MERS-CoV and SARS-CoV, SARS-CoV-2 appears to impair the maturation of dendritic cells (DCs), which is characterized by a switch in surface antigen expression. This switch enables the cells to travel to lymph nodes and activate T-cells.
To shed light on the local inflammatory infiltrate, the team compared the cell populations of professional antigen-presenting cells (APCs) in the lungs of COVID-19 autopsy cases in various stages of DAD. They found an increased number of myeloid dendritic cells (mDCs) in later stages, but with no significant upregulation of maturation markers in DAD specimens with high viral load. This accumulation of immature mDCs, which are unable to reach lymph nodes, results in an inadequate T-cell response.
Overall, this study highlights the need for further research to understand the impact of SARS-CoV-2 on the immune system and to develop more effective treatments for COVID-19Discover how the team employed digital analysis of multiplex IF images to gain insights into the unique immune profile in fatal COVID-19 cases. Investigate the potential impacts of SARS-CoV-2 and related coronaviridae on antigen-presenting cells. Learn about the role played by the UKA in COVID-19 autopsies.
-
- Experience how the team used digital analysis of multiplex IF images to learn more about the specific immune landscape in fatal COVID cases
-
- Explore the possible effects of SARS-CoV-2 and related coronaviridae on antigen presenting cells
-
- Understand the role of the UKA in COVID-19 autopsies
Prof Ralf Huss, University Hospital Augsburg
Ralf Huss, MD, PhD, is a Professor of Pathology and the Managing Deputy Director of Pathology and Molecular Diagnostics at the University Hospital in Augsburg, Germany. He is also the head of the Center for Digital Medicine.
Huss holds board certifications in anatomical, experimental, and molecular pathology and boasts over 30 years of expertise in histopathology, immunology, cancer research, and oncology.

Lukas Borcherding, Medical Student, Technical University of Munich
Lukas Borcherding is a trained nurse who has been pursuing a degree in medicine at the Technical University of Munich, Germany since 2015. In 2020-2021, he took a hiatus from his studies to concentrate on the COVID-19 pandemic and examine the unique immune profile in fatal cases. Following the completion of his project, Lukas has resumed his studies and is presently finishing the practical component of his education. Upon receiving his license, he intends to work in internal medicine.