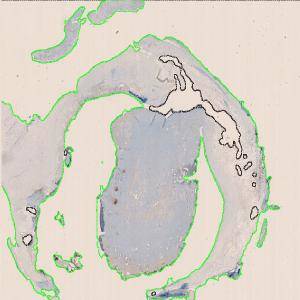
Original Image at 1x after the tissue automatically has been segmented and outlined as ROI.
#10051
This APP has been developed to quantify the occurrence of immunohistochemically detectable 5-lipoxygenase (5LO) in atherosclerotic plaques, irrespective of its cellular or extracellular location.
Lipoxygenases are a family of iron-containing enzymes that catalyze the deoxygenation of polyunsaturated fatty acids. 5LO is expressed in inflammatory cells of the myeloid line, such as histiocytes (including foam cells), dendritic reticular cells, mast cells and granulocytes. In resting myeloid cells, 5LO resides in the cytoplasm or the nucleoplasm, but when activated relocates to the nuclear membrane. 5LO is involved in the metabolism of the cell membrane derived arachidonic acid leading to formation of 4-series leukotrienes (LTs) which are major contributors to inflammatory reactions.
In arteriosclerotic disease LTs may enhance the formation of atherosclerotic plaques as well as plaque instability by effects on leukocyte chemotaxis, vascular inflammation and subsequent matrix degeneration. Important clinical endpoints have been studied in genetic association studies, where polymorphisms in the 5LO encoding gene (ALOX5) have been linked to increased risk of myocardial infarction, stroke and increased carotid intima and media thickness.
The expression of 5LO in advanced atherosclerotic plaque seems to be co-localized with CD68 positive macrophages/foam cells/dendritic reticular cells. Apart from mast cells in adventitia, other myeloid cell types contribute very little to the 5LO positive population in the arterial wall. 5LO-positive histiocytes localize to the adventitia in areas of neoangiogenesis and constitute a main component of arteriosclerotic aneurysms.
The rabbit monoclonal antibodies G590.2 (Thermo Scientific) and C49G1 (Cell Signaling) are both useful. Heat induced epitope retrieval (HIER) is mandatory; an alkaline buffer should be preferred. For the Ventana platform, HIER should be followed by a short (3-4 min) proteolytic pre-treatment.
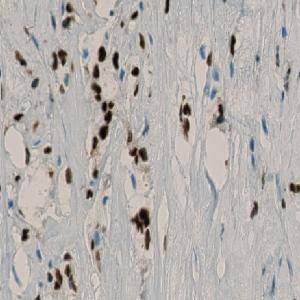
As control tissues, tonsil and liver are useful: In the tonsil, mantle zone B-lymphocytes must show a moderate nuclear reaction, and in the liver, the Kupffer cells must show a moderate cytoplasmic reaction.
Original Image at 1x after the tissue automatically has been segmented and outlined as ROI.
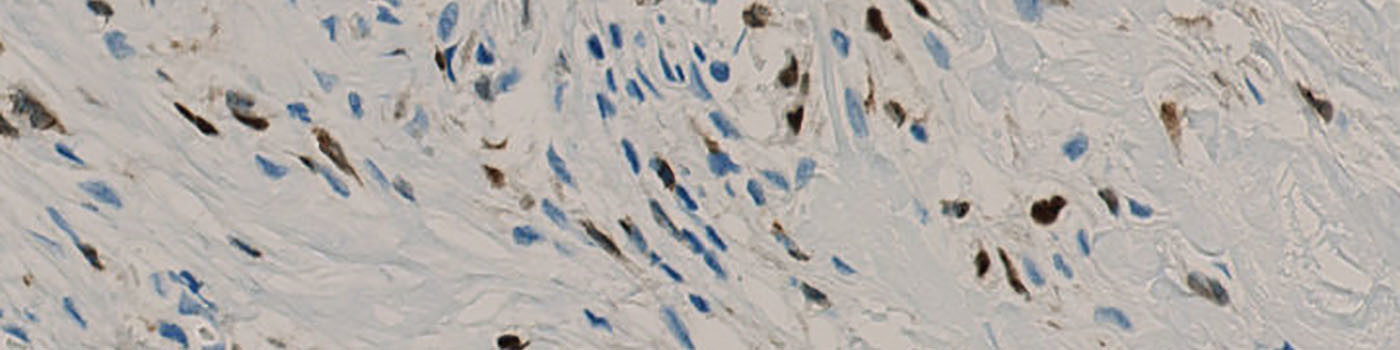
40x Field of view showing the tissue with positive and negative nuclei before segmentation.
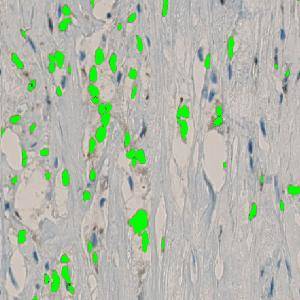
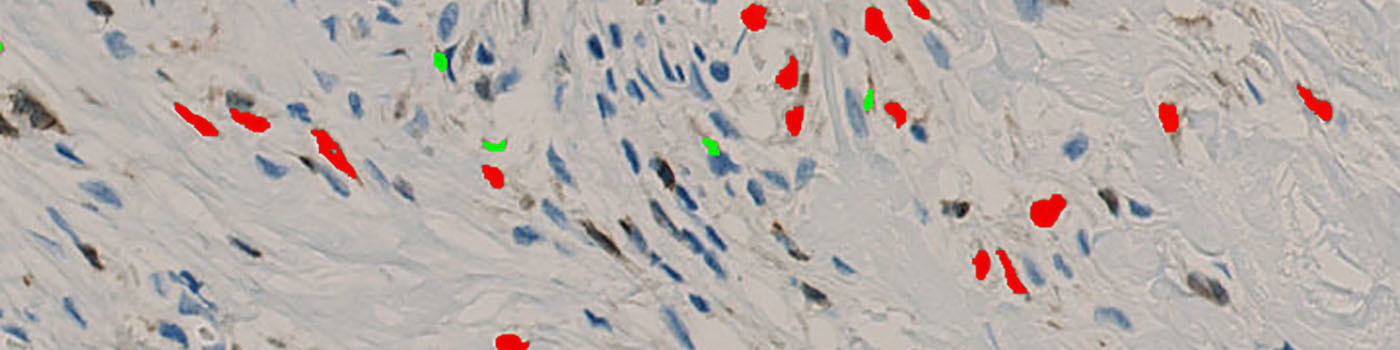
40x Field of view showing the segmented positive nuclei with a green label.
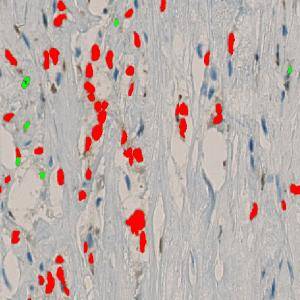
40x Field of view showing segmented positive nuclei. Green label indicating nuclei with area below 10 µm2. Red label indicating nuclei with area above 10 µm2.
Auxiliary APPs
Auxiliary APPs are used for additional process steps, e.g. finding Region of Interest (ROI).
An Auxiliary APP is used to segment and outline the tissue as ROI. The Auxiliary APP must run before the nuclei detection APP is applied.
Quantitative Output variables
Segmented nuclei are categorized in nuclei of area above and below 10 µm2. The output variables of the protocol include measurements from the two groups of nuclei and a total of these:
Methods
The first image processing step involves a segmentation of background, tissue, negative and 5LO positive nuclei (see FIGURE 3). Next a post-processing step is applied to remove background, tissue and negative nuclei (see FIGURE 4). Additionally, 5LO positive nuclei are separated into two groups based on their area (below and above 10 µm2) and nuclei with a too low staining intensity are removed. The image obtained after post-processing (see FIGURE 5) is used to determine the output variables.
Tissue is outlined as ROI automatically using an auxiliary APP. It is possible to modify the ROI outline with the layer drawing tool. This may be necessary if damaged tissue is present in the ROI.
Staining Protocol
There is no staining protocol available.
Additional information
This APP was developed in cooperation with Professor Mogens Vyberg from NordiQC and Aalborg University Hospital.
Keywords
5LO, arteriosclerosis, atherosclerotic plaques.
References
USERS
This APP was developed in cooperation with Professor Mogens Vyberg from NordiQC and Aalborg University Hospital.
LITERATURE
1. Bäck, Magnus, Inhibitors of the 5-lipoxygenase pathway in atherosclerosis, Curr Pharm Des. 2009, 15 (27), 3116-32, DOI
2. Dwyer, J.H. et. al., Arachidonate 5-lipoxygenase promoter genotype, dietary arachidonic acid, and atherosclerosis, N Engl J Med., 2004, 350 (1), 29-37, DOI
3. Cipollone, F. et. al., Association between 5-lipoxygenase expression and plaque instability in humans, Arterioscler Thromb Vasc Biol. 2005, 25 (8), 1665-70, DOI
4. Helgadottir, A. et. al., The gene encoding 5-lipoxygenase activating protein confers risk of myocardial infarction and stroke, Nat Genet. 2004, 36 (3), 233-9, DOI
5. Peters-Golden, M. et. al., Leukotrienes, N Engl J Med. 2007, 357 (18), 1841-54, DOI
6. Qiu, H. et. al., Expression of 5-lipoxygenase and leukotriene A4 hydrolase in human atherosclerotic lesions correlates with symptoms of plaque instability, Proc Natl Acad Sci USA 2006, 103 (21), 8161-6, DOI
7. Spanbroek, R. et. al., Expanding expression of the 5-lipoxygenase pathway within the arterial wall during human atherogenesis, Proc Natl Acad Sci USA 2003, 100 (3), 1238-43, DOI
8. Zhao, L. et. al., Lipoxygenase pathways in atherogenesis, Trends Cardiovasc Med. 2004, 14 (5), 191-5, DOI
9. Zhao, L. et. al., The 5-lipoxygenase pathway promotes pathogenesis of hyperlipidemia-dependent aortic aneurysm, Nat Med Sep 2004, 10 (9), 966-73, DOI